A stalled scale or a stuck lift is a symptom, not a diagnosis. The same outcome can come from very different mechanisms, and the response that resolves a plateau depends entirely on identifying which one is actually driving it.
Training and nutrition plateaus fall into four categories with distinct mechanisms and signs. Physiological plateaus include caloric adaptation, where a fixed intake produces a progressively smaller deficit as bodyweight falls, and accumulated fatigue, where fatigue accumulates faster than fitness causing expressed performance to decline. Nutritional plateaus include protein insufficiency, inadequate carbohydrate availability relative to training demand, and micronutrient deficiencies in iron, vitamin D, zinc, or magnesium. Programming plateaus include genuine progressive overload failure and program stagnation, though both are less common than assumed and most resolve with improved tracking rather than program replacement. Psychological plateaus include diet fatigue, where prolonged restriction erodes adherence, and training monotony, where repetitive sessions reduce motivation and session quality. Ruling out physiological and nutritional causes before attributing a plateau to programming or psychology produces more accurate diagnoses and more effective responses.

Plateaus are one of the most common and most mishandled challenges in training and body composition. The default response tends to be to change everything: cut more calories, add more cardio, switch programs, try a new supplement stack. This approach occasionally works by accident, but it works for the wrong reasons, and it forfeits the understanding of what actually caused the plateau that would make the next phase more effective.
The framework here sorts the nine most common plateau mechanisms into four categories: physiological, nutritional, programming, and psychological. Each category has a distinct set of causes, signs, and appropriate responses. Matching the response to the actual mechanism is what makes the difference between a productive adjustment and a month of increased effort that produces no additional result.
One important caveat before the categories are covered: these mechanisms overlap significantly in how they present on the surface. Caloric adaptation and diet fatigue can look almost identical from the outside. Accumulated fatigue and protein insufficiency produce similar performance symptoms. The signs listed for each are starting points for investigation rather than definitive diagnoses, and in many cases more than one mechanism is contributing simultaneously.
What Causes Physiological Plateaus?
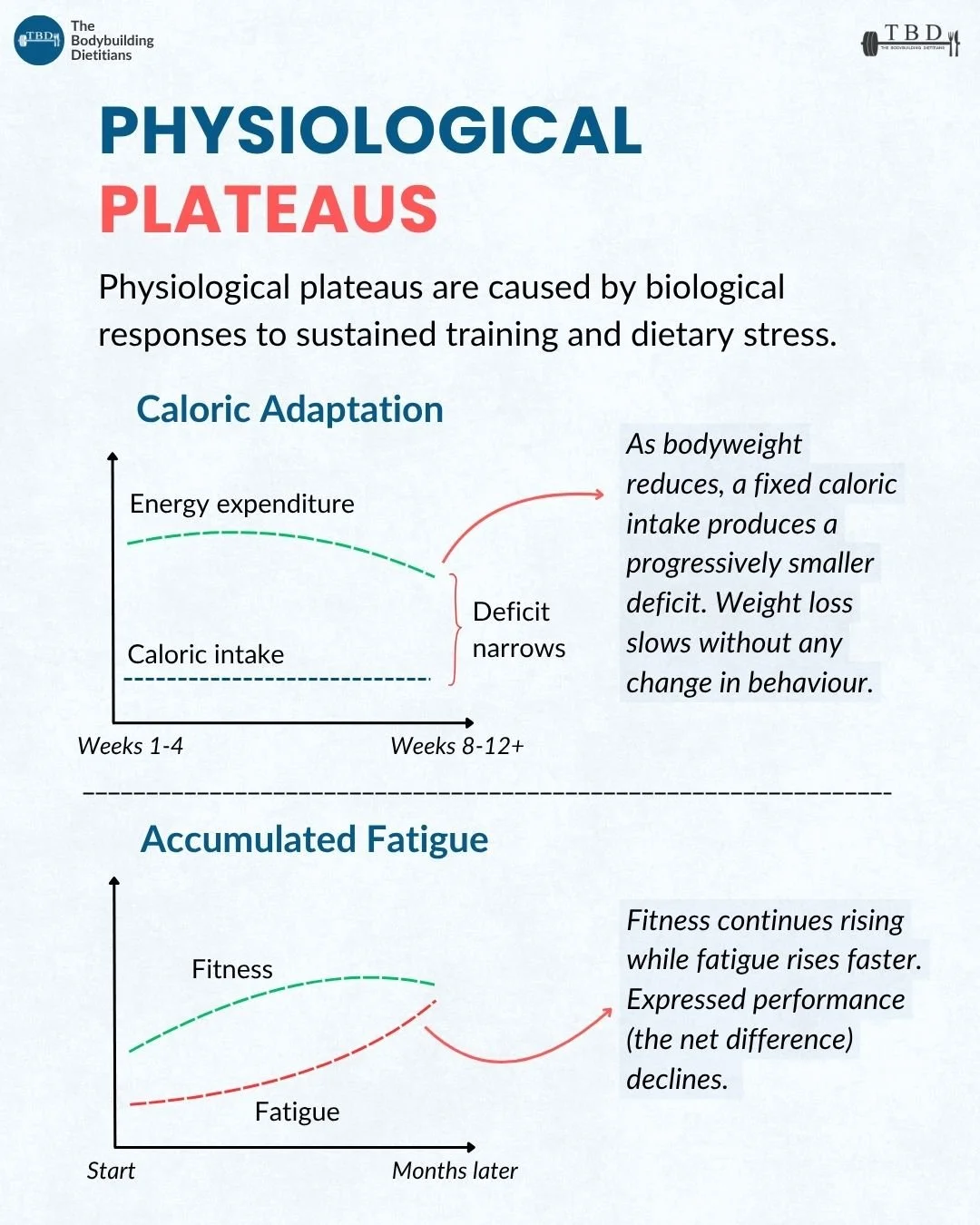
Physiological plateaus are caused by biological responses to sustained training and dietary stress. They are not signs of failure or the consequence of doing something wrong. They are adaptive processes the body runs in response to the demands being placed on it, and understanding them as such changes how productively someone responds.
Caloric adaptation: As bodyweight decreases during a fat loss phase, total daily energy expenditure falls through several mechanisms: basal metabolic rate declines in proportion to the smaller body mass, adaptive thermogenesis reduces metabolic rate beyond what mass loss predicts, and NEAT declines automatically as the body conserves energy. The consequence is that a fixed calorie intake, which produced a meaningful deficit at the start of a diet, produces a progressively smaller deficit over weeks and months, until weight loss slows or stalls entirely without any change in dietary behaviour.
The signs of caloric adaptation include a stalled scale across two to three weeks with consistent adherence, increasing hunger and declining energy levels, and a general sense of effort that feels disproportionate to what the calorie intake should theoretically be producing. The response is not to conclude that the diet has stopped working, but to recognise that the maintenance calorie level has moved. A modest reduction in intake, an increase in energy expenditure through activity, or a structured diet break followed by a recalibrated approach are all appropriate responses depending on where the individual is in their dieting phase.
Adaptive thermogenesis is the reduction in total daily energy expenditure during sustained calorie restriction that exceeds what is predicted from mass loss alone. It is one of the body's primary mechanisms for defending against prolonged energy deficit and is a consistent feature of fat loss phases beyond the early weeks.
Accumulated fatigue: In exercise physiology, the relationship between fitness and fatigue determines expressed training performance. Fitness and fatigue both accumulate during a training block, but fatigue is more acute and shorter-lived than fitness, which means that when fatigue accumulates faster than it dissipates between sessions, expressed performance declines even as underlying fitness continues to improve. This is the physiological basis for periodised deload periods in structured training programs.
The signs of accumulated fatigue are distinct from simple underrecovery on a given day: performance declining across multiple sessions, persistent muscle soreness that does not resolve within normal recovery windows, disrupted sleep, elevated resting heart rate, and a general heaviness that makes training feel harder at loads that were recently manageable. A structured deload period, typically one to two weeks of reduced training volume while maintaining intensity, allows fatigue to dissipate and fitness to be expressed again.
What Causes Nutritional Plateaus?
Nutritional plateaus arise when dietary intake no longer meets the demands that training and the current phase of dieting are placing on the body. They are particularly relevant during fat loss phases, where the combination of reduced total food intake and increased training stress creates conditions in which multiple nutritional variables can fall short simultaneously.
Protein insufficiency: Protein requirements increase during a calorie deficit, because the body's tendency to use amino acids for energy accelerates when total energy is restricted and glycogen availability is reduced. When protein intake is insufficient relative to that elevated requirement, lean mass is progressively lost alongside fat during a deficit, blunting the body composition outcome of the diet and reducing the training stimulus available to preserve muscle tissue.
The signs of protein insufficiency in a dieting context include declining strength that is disproportionate to the stage of the diet and the calorie deficit in place, delayed recovery between sessions, and gradual reduction in lean mass confirmed through body composition assessment. Protein targets of 2.0 to 2.4 grams per kilogram of bodyweight during a deficit are well-supported in the literature for preserving lean mass in resistance-trained individuals. Confirming that actual intake is consistently meeting this target, rather than assuming it is, is the appropriate first step.
Carbohydrate availability: Chronically low carbohydrate intake relative to training demand reduces the glycogen availability that high-intensity resistance training relies on as its primary fuel source. This can produce a training performance decline and elevated cortisol that are independent of total calorie intake, meaning that even in a diet where total macros are ostensibly appropriate, the specific distribution of carbohydrate relative to training load may be limiting output.
The signs of insufficient carbohydrate availability include declining training volume capacity, fatigue within sessions that feels disproportionate to the load and volume being performed, a subjective heaviness that does not resolve between sessions, and in some cases elevated irritability reflecting cortisol elevation. Structuring carbohydrate intake around training, with the largest carbohydrate allocation concentrated in the pre-workout and post-workout meals, is the standard practical response.
Micronutrient insufficiency: Deficiencies in iron, vitamin D, zinc, and magnesium are among the more common nutritional findings in resistance-trained individuals, and they become more likely to emerge or worsen during sustained periods of calorie restriction when food volume and variety decrease. Critically, the symptoms they produce, fatigue, poor recovery, declining performance, and hormonal disruption, closely mimic the signs of other plateau causes, which makes them genuinely difficult to attribute correctly without objective measurement.
Bloodwork is the most reliable diagnostic tool for identifying micronutrient insufficiency and is worth including in a monitoring framework for anyone in an extended fat loss phase or contest prep. Attributing performance decline to overtraining or caloric adaptation when the actual cause is iron deficiency or insufficient vitamin D leads to interventions that do not address the problem.
What Causes Programming Plateaus?
Programming plateaus occur when the training stimulus is no longer sufficient to drive further adaptation. They are genuine and they do occur, but they are also considerably less common than most people experiencing a plateau assume, because the physiological and nutritional causes covered above are more frequent and share similar presentations.
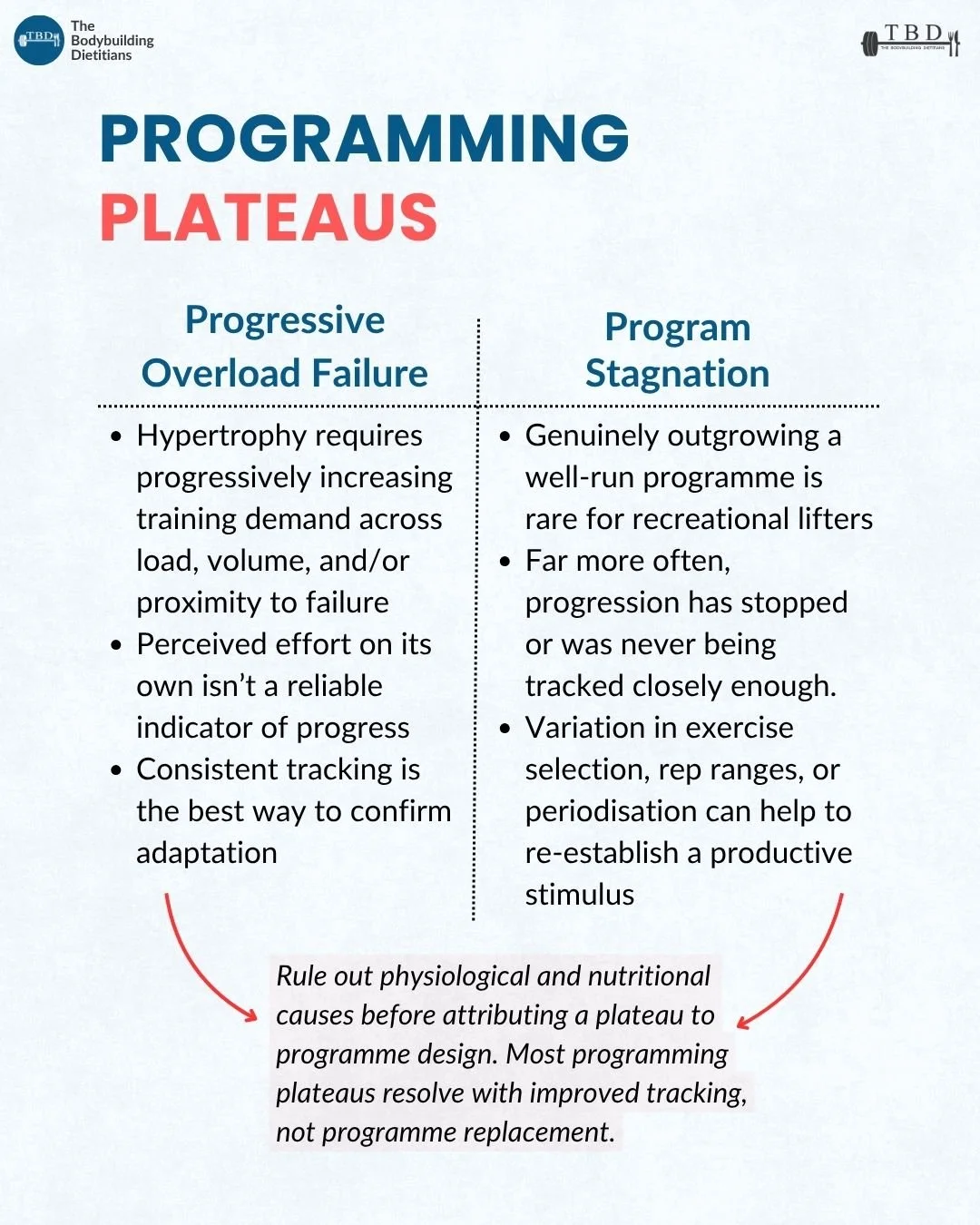
Progressive overload failure: Hypertrophy and strength adaptation require the progressive increase of training demand over time across load, volume, or proximity to failure. When this progression stops, the training stimulus is no longer sufficient to drive further adaptation, and progress plateaus.
The challenge is that perceived effort is not a reliable indicator of whether progressive overload is being achieved. A session that feels hard may produce identical load and volume to the previous three sessions if no structured attempt has been made to increase either. Consistent tracking of load, sets, reps, and subjective intensity across sessions is the practical mechanism through which progressive overload is confirmed rather than assumed.
The appropriate first response to apparent progressive overload failure is to verify the training data: has load or volume actually failed to increase across multiple weeks, or has the tracking been insufficiently detailed to confirm it? In many cases, perceived plateaus in overload resolve when tracking is made more rigorous rather than when the program is changed.
Program stagnation: Genuinely outgrowing a well-designed and consistently followed program is rarer than the culture around program-hopping suggests, and for most recreational lifters it is not the limiting factor. The more common pattern is that progression has stopped for physiological or nutritional reasons, and the program is being held responsible for an outcome it did not cause.
When adaptation genuinely plateaus despite confirmed progressive overload and adequate nutritional support, variation in exercise selection, rep ranges, periodisation structure, or training frequency can re-establish a more productive stimulus. The principle here is that a different stimulus, applied to the same muscle groups with the same progressive overload intent, can recruit different motor unit populations and produce adaptation that the previous configuration was not generating.
The practical note from the carousel is worth repeating: rule out physiological and nutritional causes before attributing a plateau to program design. Most programming plateaus resolve with improved tracking rather than program replacement.
What Causes Psychological Plateaus?
Psychological plateaus are caused by the erosion of the behavioural consistency that makes a training and nutrition plan productive. They are not a reflection of inadequate motivation or character. They are predictable responses to the specific demands of prolonged dietary restriction and repetitive training, and they respond to structural interventions rather than exhortations to try harder.
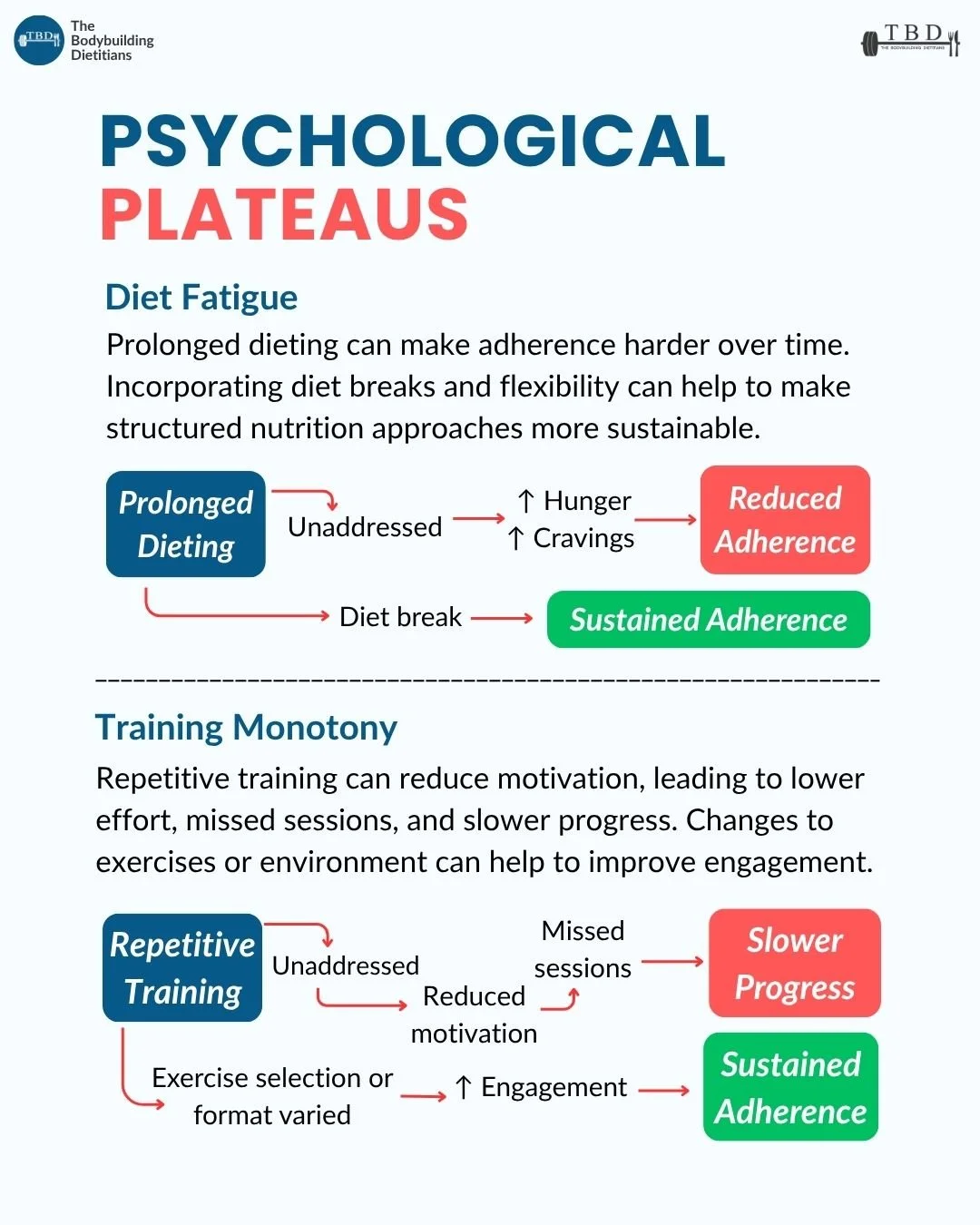
Diet fatigue: Prolonged dietary restriction produces a predictable accumulation of physiological and psychological signals that make adherence progressively harder over time. Rising ghrelin, falling leptin, elevated cortisol, declining mood, and the cognitive burden of continuous dietary regulation all contribute to a state where the effort required to maintain the diet exceeds what the individual can sustain consistently. The result is not a sudden failure of willpower but a gradual erosion of the dietary adherence that was producing progress.
In the context of plateau diagnosis, the relevant signal is adherence that has become inconsistent not because of poor planning or external disruption but because maintaining dietary restraint has become more effortful than it was earlier in the phase. The appropriate response is a structured diet break of one to two weeks at maintenance calories, which partially restores the hormonal environment and psychological tolerance for continued restriction.
Training monotony: Repetitive training, performing the same exercises in the same format across many consecutive weeks or months, can progressively reduce the engagement and intrinsic motivation that sustain consistent session effort and attendance. The consequence is not necessarily conscious avoidance but a gradual decline in the intensity of effort brought to each session and an increasing frequency of skipped or shortened sessions that accumulate into slower progress over time.
The response to training monotony is structural variation rather than motivational intervention. Changes to exercise selection, training format, session structure, or training environment can restore engagement and re-establish the consistent high-quality effort that plateau recovery requires. This does not mean abandoning progressive overload principles. It means applying them through a changed exercise or format that provides a more engaging training stimulus.
The interaction between diet fatigue, training monotony, and overall adherence to a long-phase plan is worth addressing explicitly in the context of contest prep and extended fat loss phases, where both are likely to emerge simultaneously and compound each other. Managing both with appropriate planned variation is part of how our coaching clients navigate longer phases without the cumulative adherence erosion that derails otherwise sound approaches.
How Should These Categories Be Used in Practice?
The framework is a diagnostic starting point rather than a decision tree. The practical process for working through a plateau follows a logical order: confirm what is actually stalled and for how long, assess the signs most consistently present across the relevant categories, rule out the more common and more consequential causes before attributing the plateau to less common ones, and match the response to the identified mechanism.
Physiological causes should generally be considered first because they are the most common in individuals who are genuinely adhering to their plan, and because the appropriate response to caloric adaptation or accumulated fatigue is different from the response to overload failure or diet fatigue. The signs across categories do overlap, which makes the order of investigation matter.
Nutritional causes are worth considering in parallel with physiological ones, particularly for individuals in extended deficits or contest prep where protein, carbohydrate, and micronutrient status are all under greater pressure than in a standard training context. Bloodwork provides information that no amount of subjective assessment can substitute for when micronutrient insufficiency is suspected.
Programming causes are appropriate to consider once physiological and nutritional factors have been addressed or ruled out. Changing the program before confirming that the program is the problem is one of the more common and more costly errors in plateau management, because it removes potentially productive stimulus in response to a cause the program change cannot address.
Psychological causes typically become relevant in longer phases and are worth monitoring continuously rather than addressing only when they become acute. Planned diet breaks and intentional variation in training format are more effective as proactive management tools than reactive responses to a crisis of adherence.
Practical Takeaways
A plateau is a symptom, not a diagnosis. The same presenting sign, a stalled scale or a stuck lift, can arise from nine distinct mechanisms across four categories, and the appropriate response depends on which one is actually driving it.
Physiological plateaus come from biological adaptation. Caloric adaptation narrows the deficit over time as bodyweight and metabolic rate fall. Accumulated fatigue masks underlying fitness gains and depresses expressed performance.
Nutritional plateaus arise when intake no longer meets demand. Protein requirements increase in a deficit. Carbohydrate availability affects training output independent of total calories. Micronutrient deficiencies produce fatigue and performance impairment that closely mimic other plateau causes, and bloodwork is the most reliable way to confirm them.
Programming plateaus are less common than assumed. Genuinely outgrowing a well-designed program is rare. Most programming plateaus resolve with improved tracking rather than program replacement, and physiological and nutritional causes should be ruled out before attributing a plateau to the program.
Psychological plateaus come from the demands of prolonged dieting and repetitive training. Diet fatigue erodes adherence through accumulating physiological and psychological signals. Training monotony reduces engagement and session quality. Both respond to structural variation: diet breaks and intentional exercise or format changes respectively.
These categories overlap in presentation. The signs are starting points for investigation rather than definitive diagnoses, and multiple mechanisms often contribute simultaneously.
Frequently Asked Questions
Why has my weight loss stalled even though I am still dieting?
A stalled scale during a consistent calorie deficit is most often explained by caloric adaptation, the narrowing of the energy deficit that occurs as bodyweight and metabolic rate fall during sustained restriction. A fixed calorie intake that produced a meaningful deficit at the start of a diet produces a progressively smaller deficit as weight decreases and the body adapts. A modest reduction in calorie intake, an increase in daily movement, or a structured diet break followed by a recalibrated approach are the appropriate responses, depending on where the individual is in the phase.
How do I know if my plateau is from overtraining or not eating enough?
Accumulated fatigue and protein insufficiency both produce performance decline and poor recovery, which makes them difficult to distinguish by symptoms alone. Accumulated fatigue tends to be associated with a recent increase in training volume or a prolonged training block without an adequate deload, and typically resolves with a structured reduction in training volume. Protein insufficiency is associated with declining strength and increasing recovery time during a calorie deficit, and is confirmed by auditing actual daily protein intake against the target. Both can be present simultaneously, particularly in athletes managing aggressive fat loss phases.
Should I change my program when progress stalls?
Program change is appropriate when genuine progressive overload failure has been confirmed through consistent tracking over multiple weeks and physiological and nutritional causes have been addressed or ruled out. Before changing a program, it is worth confirming that load and volume have actually stopped increasing rather than assuming they have, since perceived effort is not a reliable indicator of objective progression. Most apparent programming plateaus resolve with improved tracking, a deload, or nutritional adjustments rather than program replacement.
What micronutrient deficiencies most commonly affect training performance?
Iron, vitamin D, zinc, and magnesium are among the most commonly identified deficiencies in resistance-trained individuals during fat loss phases. Iron deficiency, even without anaemia, can produce significant fatigue and reduced endurance capacity. Vitamin D insufficiency is associated with reduced muscle function, immune impairment, and mood disruption. Magnesium plays roles in muscle contraction, sleep quality, and stress response. Zinc is involved in testosterone production and immune function. All of these produce symptoms that overlap with other plateau causes, which is why bloodwork rather than symptom assessment alone is the most reliable diagnostic approach.
How long should a diet break be to address a plateau?
A structured diet break of approximately one to two weeks at maintenance calories is the standard recommendation for addressing caloric adaptation and diet fatigue. This duration allows partial restoration of leptin, some normalisation of cortisol, glycogen replenishment, and a meaningful recovery of the psychological tolerance required to sustain continued restriction. A diet break that is too short, less than five to seven days, may not provide sufficient recovery of the hormonal environment to produce the intended benefit. After the break, intake is reduced back below maintenance and the diet resumes, ideally with a recalibrated maintenance estimate based on current bodyweight.
Is it possible to have multiple plateau causes at once?
Yes, and it is common, particularly in extended fat loss phases and contest prep. Caloric adaptation and diet fatigue frequently co-exist, because both are consequences of prolonged energy restriction. Accumulated fatigue and carbohydrate insufficiency similarly overlap in their mechanisms and signs. The framework is intended to prompt systematic assessment of each category rather than to imply mutual exclusivity between them. Identifying the most prominent contributing mechanism and addressing it first, while monitoring for others, is a more productive approach than attempting to resolve all possible causes simultaneously.
Working out which mechanism is actually driving a plateau, rather than changing everything at once and hoping, is a large part of what our one-on-one coaching involves. If you want support diagnosing and addressing a stall in your training or body composition progress, you can enquire about coaching or book a consultation to get started.