Bowel cancer incidence has been rising steadily in adults under 50 for two decades, while it has fallen substantially in adults over 50. A dietitian walks through what the evidence suggests is driving the shift, and the practical dietary and lifestyle habits that consistently show up as protective across large prospective studies.
Bowel cancer incidence in adults under 50 has been rising for two decades in Australia and other high-income countries, with the increase most pronounced in the 30 to 39 age group. In the United States, colorectal cancer became the leading cause of cancer death in adults under 50 in 2023, arriving seven years earlier than previously projected. The exact cause of the rise remains unclear but current evidence points to a combination of dietary and lifestyle changes that have compounded across generations, including higher ultra-processed food intake, reduced physical activity, higher obesity rates, altered gut microbiome composition, and sustained alcohol consumption in younger cohorts. The protective factors that appear most consistently across large prospective studies are higher dietary fibre intake (particularly from legumes, oats, vegetables, and wholegrains), regular physical activity, maintenance of healthy body composition, lower processed meat intake, and reduced alcohol consumption. None of these guarantee prevention, but they are the modifiable variables that current evidence supports acting on. Screening guidelines in Australia and the US have been lowered to age 45 to reflect the shift toward earlier presentation.
Bowel cancer, also known as colorectal cancer, has undergone a striking generational shift over the past two decades. In older adults, incidence rates have fallen significantly, largely due to expanded screening programs and improved detection. In younger adults, the trend has moved in the opposite direction, with new diagnoses climbing steadily across every age group under 50 in Australia and most other high-income countries.
The purpose of this article is to walk through what the current evidence shows about why this shift is happening, and what the research literature identifies as the most consistently protective dietary and lifestyle factors. Much of what will follow is associational rather than causal, and the actual mechanism behind the rising rates in younger cohorts is likely to involve several factors interacting rather than a single identifiable cause. What the literature does support with more confidence is the direction of the modifiable variables, and those are the practical levers this article focuses on.
What Is the Trend, and How Significant Is It?
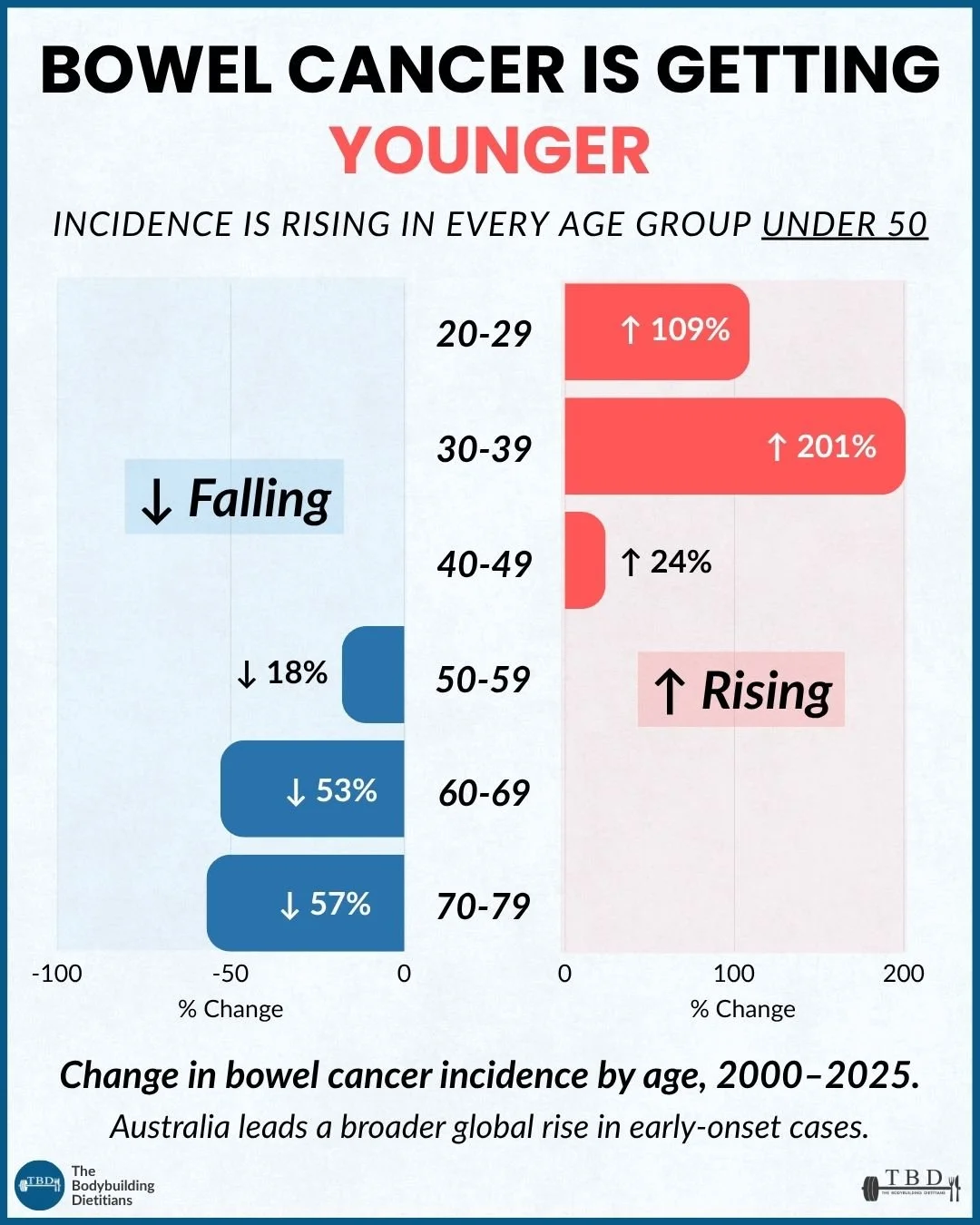
Bowel cancer incidence in adults under 50 has been rising steadily in Australia and other high-income countries since around 2000, with the increase most pronounced in the 30 to 39 age group. Over the same period, rates in adults over 50 have fallen substantially, largely due to expanded screening programs and improved early detection.
The Australian data shows the shift clearly. Between 2000 and 2025, colorectal cancer incidence rates in adults under 50 have risen across every age group, with the sharpest rises in the 20 to 29 and 30 to 39 cohorts. Rates in adults 50 and over have fallen by 18 percent (age 50 to 59), 53 percent (age 60 to 69), and 57 percent (age 70 to 79) over the same period.
Data from the Australian Institute of Health and Welfare shows that between 2000 and 2024, the number of colon cancer cases diagnosed in Australians under 50 more than doubled, from 585 cases to an estimated 1,352 cases. The colorectal cancer incidence rate in people under 50 increased from 7 to an estimated 12 cases per 100,000 people, while rates in the 50-plus population declined substantially over the same period due to the National Bowel Cancer Screening Program and improved detection. Source: Australian Institute of Health and Welfare, Cancer Data in Australia 2025.
The picture in the United States is similar and, in some respects, more advanced. Colorectal cancer became the leading cause of cancer death in adults under 50 in the US in 2023, arriving seven years earlier than the projection published a few years prior. In 1990, colorectal cancer was the fifth-leading cause of cancer death in this age group.
A research letter analysing National Cancer Institute data found that colorectal cancer mortality in Americans under 50 increased by 1.1 percent per year since 2005, moving it from the fifth-leading cause of cancer death in this age group in the early 1990s to the leading cause of cancer death in men and women combined by 2023. This was the only cause of cancer death to increase in the under-50 population over this period. Source: Siegel et al., 2026, JAMA, 335(7):632-634.
Australia, the United Kingdom, Canada, and New Zealand are all reporting similar upward trends in younger cohorts. The rise is not confined to high-income countries and has now been documented across a broad range of populations.
In Australia, screening guidelines were revised in 2024 to lower the age of eligibility for the National Bowel Cancer Screening Program to 45 (from 50 previously), reflecting the increased incidence in younger cohorts. The United States lowered its recommended screening age to 45 in 2018 for similar reasons.
Why Are Rates Rising in Younger Adults?
The exact cause of the rising incidence in younger cohorts remains unclear, and this is one of the more active areas of ongoing research in cancer epidemiology. What current evidence points to is a combination of dietary and lifestyle changes that have compounded across generations, rather than a single identifiable cause.
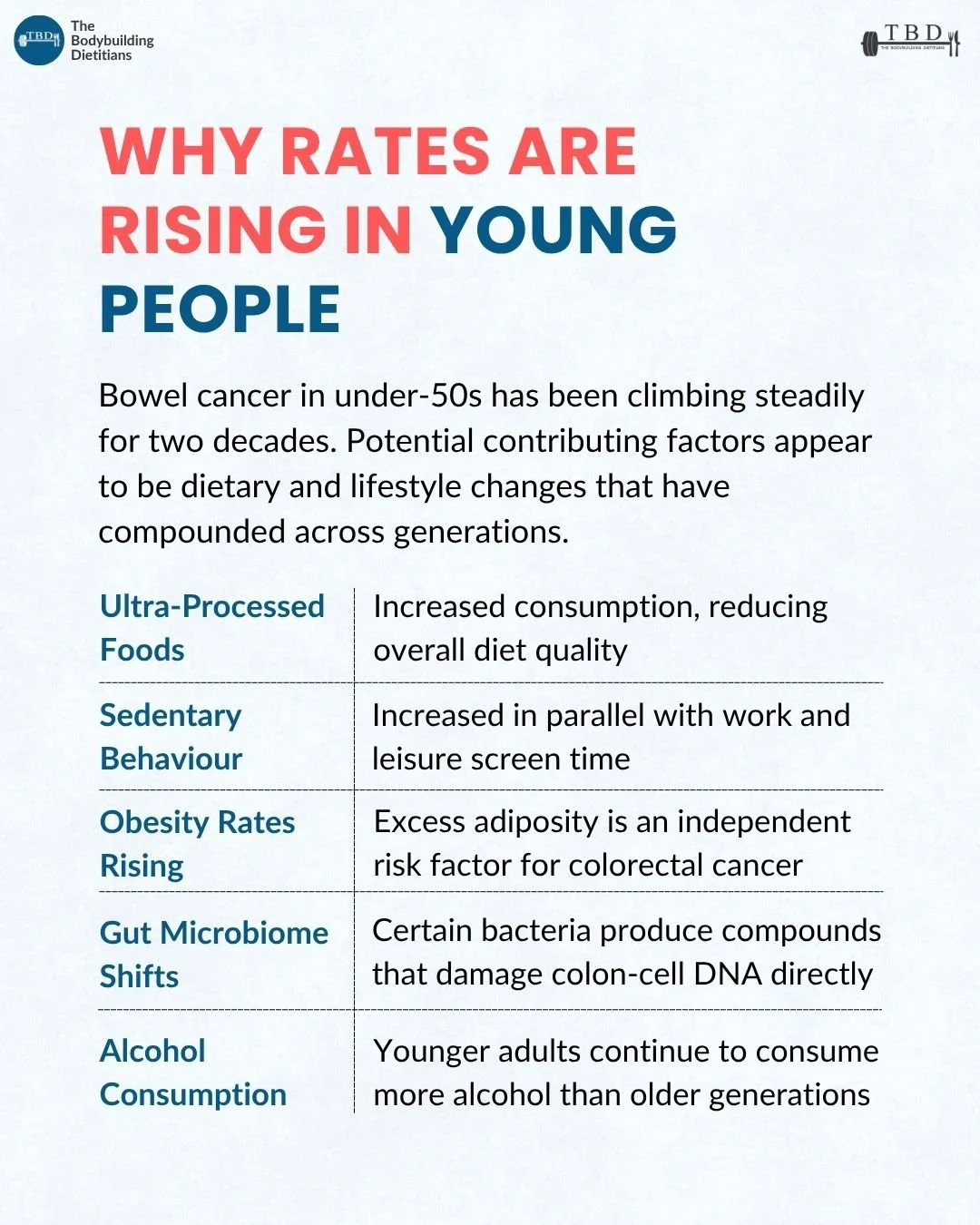
Five factors appear consistently in the research literature as potential contributors:
Ultra-processed food consumption has increased substantially in high-income countries over the past several decades, particularly in the diets of children and adolescents born after the 1980s. Higher ultra-processed food intake is associated with reduced overall diet quality, lower fibre intake, altered gut microbiome composition, and increased inflammation. Each of these has been separately linked to colorectal cancer risk in observational studies.
Sedentary behaviour has increased in parallel with work and leisure screen time. Prolonged sitting is associated with reduced intestinal transit time, higher circulating insulin levels, and increased inflammation, all of which are plausible mechanisms for increased colorectal cancer risk.
Obesity rates have risen substantially across all age groups but particularly in younger cohorts. Excess body fat, particularly visceral fat, is an independent risk factor for colorectal cancer through effects on circulating insulin, insulin-like growth factor 1 (IGF-1), and inflammatory markers.
Gut microbiome composition has shifted in populations consuming Western-style diets, with reduced microbial diversity, altered species composition, and changes in the balance of bacterial metabolites. Some bacterial species produce compounds (including colibactin from certain strains of Escherichia coli) that can damage colon-cell DNA directly, and shifts in microbial composition have been implicated in colorectal cancer development.
Alcohol consumption in younger adults has remained higher than in older generations in some regions, and alcohol is a well-established risk factor for colorectal cancer with no clearly established safe threshold.
Most of the evidence linking these factors to the rise in early-onset colorectal cancer is associational at this stage. The true mechanism is likely to involve several of these factors interacting rather than a single cause, and specific individual risk depends on genetic, familial, and environmental factors that cannot be captured by population-level trend data. What the literature does support with more confidence is the direction of the modifiable variables, and those are the practical levers this article covers next.
For a more detailed look at how gut microbiome shifts are shaped by dietary and lifestyle inputs, our article on gut health walks through the eight variables that most influence digestive function and microbial composition.
How Does Fibre Reduce Colorectal Cancer Risk?
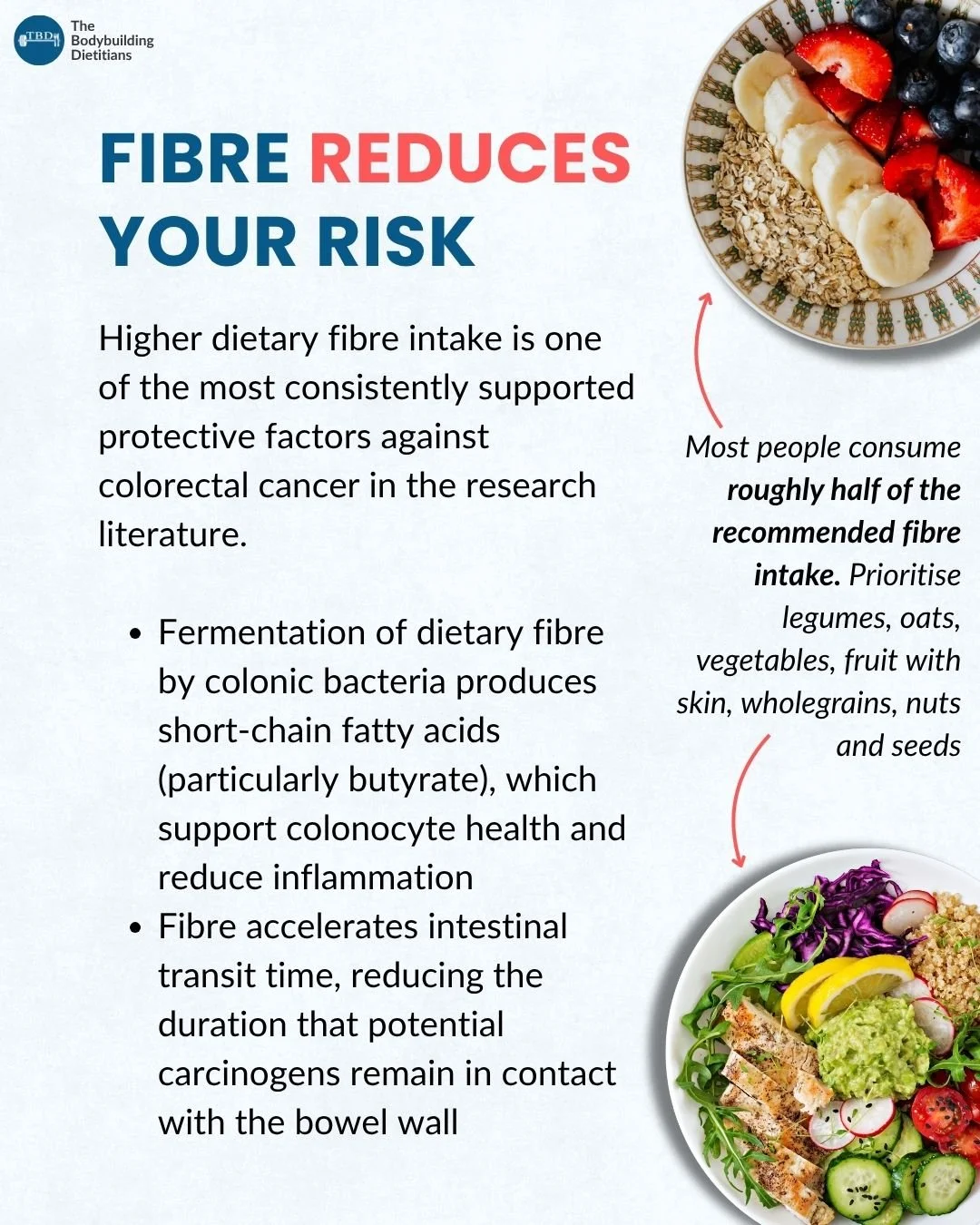
Higher dietary fibre intake is one of the most consistently supported protective factors against colorectal cancer in the research literature. Two mechanisms account for most of the observed protective effect.
The first is the fermentation of dietary fibre by colonic bacteria into short-chain fatty acids (SCFAs), particularly butyrate. Butyrate is the primary energy source for colonocytes (the cells lining the colon) and plays a central role in maintaining the intestinal barrier, modulating local immune responses, and regulating inflammation. Higher SCFA production supports a healthier colonic environment and reduces several pathways implicated in colorectal cancer development.
The second is that fibre accelerates intestinal transit time, reducing the duration that potential carcinogens (from diet, from bacterial metabolism of certain compounds, or from other sources) remain in contact with the bowel wall. Faster transit means less prolonged exposure of the colonic epithelium to potentially damaging compounds.
A comprehensive meta-analysis of prospective cohort studies found that higher dietary fibre intake, particularly from whole grains and cereals, was associated with a reduced risk of colorectal cancer. Each additional 10 grams of dietary fibre per day was associated with a 10 percent reduction in colorectal cancer risk in the pooled analysis. Source: Aune et al., 2011, BMJ, 343:d6617.
The Australian recommended daily fibre intake is 25 grams for women and 30 grams for men, and most adults consume roughly half of this. The gap between typical and recommended intake represents one of the more achievable dietary levers for reducing colorectal cancer risk, and it is one that also produces observable improvements in digestive comfort, satiety, and blood glucose control within weeks.
Practical sources of dietary fibre that show up consistently in the research as most protective include legumes (lentils, chickpeas, kidney beans, black beans), oats and other whole grains, vegetables (particularly cruciferous vegetables like broccoli, cauliflower, and brussels sprouts), fruit with skin (apples, pears, berries), nuts and seeds. A daily intake pattern that includes a serving of legumes, oats or another whole grain, several servings of vegetables, and a serving or two of fruit reliably reaches or exceeds the recommended range.
How Do Processed and Red Meat Affect Colorectal Cancer Risk?
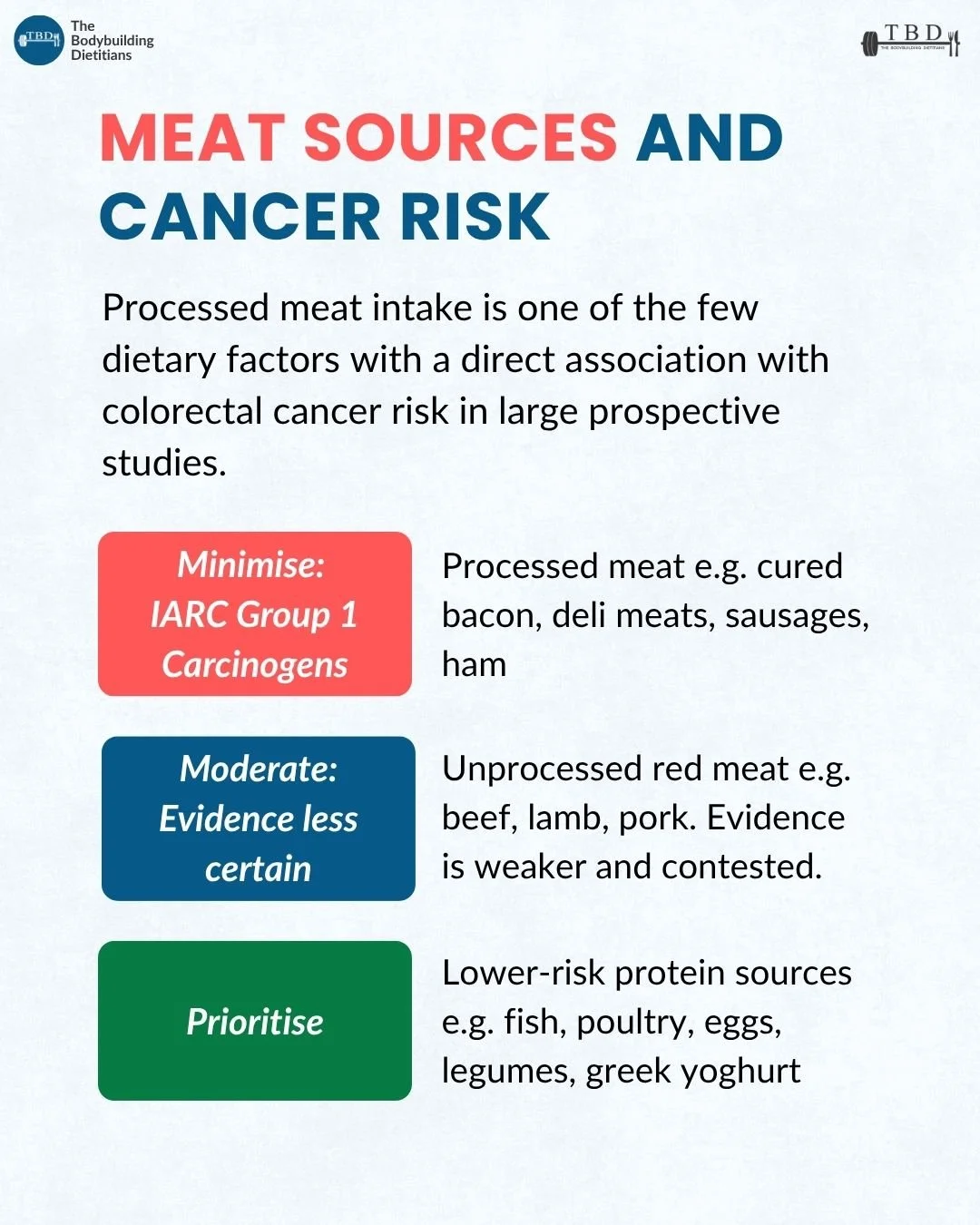
Processed meat intake is one of the few dietary factors with a direct association with colorectal cancer risk in large prospective studies, and the evidence is strong enough that the International Agency for Research on Cancer classified processed meat as a Group 1 carcinogen in 2015 (the same category as tobacco smoking and asbestos, based on strength of evidence for causation rather than magnitude of risk).
The International Agency for Research on Cancer working group evaluated over 800 studies on the association between meat consumption and cancer and concluded that consumption of processed meat is carcinogenic to humans (Group 1) based on sufficient evidence in humans that consumption causes colorectal cancer. Each 50-gram portion of processed meat consumed daily was associated with an approximately 18 percent increase in colorectal cancer risk in the pooled analysis. Source: Bouvard et al., 2015, Lancet Oncology, 16(16):1599-1600.
Processed meat includes cured bacon, deli meats (ham, salami, mortadella), sausages, hot dogs, and other meats preserved through smoking, curing, salting, or the addition of preservatives. The mechanism is thought to involve compounds formed during the processing itself (nitrites, nitrates, N-nitroso compounds) and compounds formed when the meat is cooked at high temperatures (heterocyclic amines, polycyclic aromatic hydrocarbons).
The evidence on unprocessed red meat is weaker and more contested. IARC classified red meat as a Group 2A carcinogen (probably carcinogenic to humans) based on limited evidence in humans and strong mechanistic evidence, but the magnitude of any effect is smaller than for processed meat, and some larger recent analyses have not found statistically significant associations at moderate intakes. The World Cancer Research Fund suggests limiting unprocessed red meat to approximately 500 grams (cooked weight) per week, which corresponds to roughly three to four servings of red meat per week.
The practical framework that emerges from this evidence is to minimise processed meat where possible, keep unprocessed red meat in a moderate range (in line with the WCRF guidance or below), and prioritise lower-risk protein sources including fish, poultry, eggs, legumes, tofu, and dairy products including Greek yoghurt. This does not require complete elimination of any category. A daily bacon habit and a weekend steak are different orders of magnitude of risk exposure, and the practical adjustment is usually about frequency rather than absolute avoidance.
For lifters and physique athletes who rely on higher protein intakes, this is a relevant consideration when planning protein sources across the week. For a more detailed look at how different protein sources compare on amino acid composition and practical value, our article on protein metabolism covers the underlying framework.
How Do Body Composition and Physical Activity Influence Risk?
Body composition and physical activity operate as two of the most important non-dietary risk factors for colorectal cancer, with effects that partially overlap and partially operate through independent pathways.
Body composition influences colorectal cancer risk primarily through the effects of excess body fat on circulating hormones and inflammatory markers. Higher body fat, particularly visceral fat, is associated with elevated circulating insulin, higher IGF-1 levels, and increased levels of pro-inflammatory cytokines. Each of these operates as an independent pathway in colorectal cancer promotion: insulin and IGF-1 are growth-promoting signals that support cell proliferation, and chronic low-grade inflammation contributes to the tissue environment in which cancer can develop.
Body weight itself is a meaningful risk factor, operating separately from dietary composition. Two individuals with similar diet quality but meaningfully different body composition can have different colorectal cancer risk profiles, driven by the metabolic effects of the excess fat mass itself. This means that improving body composition is a modifiable variable that produces risk reduction beyond what dietary changes alone provide.
Physical activity reduces colorectal cancer risk through multiple mechanisms, including reduced intestinal transit time, improved insulin sensitivity, lower systemic inflammation, and effects on immune function. Regular exercise is associated with meaningful risk reduction in prospective studies, with both aerobic and resistance training contributing.
A meta-analysis of prospective studies found that physically active individuals had approximately 20 to 25 percent lower colon cancer risk compared to sedentary individuals. The protective effect was independent of body mass index and was observed for both aerobic activity and resistance training. Source: Wolin et al., 2009, British Journal of Cancer, 100(4):611-616.
The practical implication is that maintaining a healthy body composition and engaging in regular physical activity are two of the most consistently effective non-dietary levers for reducing colorectal cancer risk. For lifters and physique-focused readers, this is an additional layer of context for a training and body composition approach that is already central to their goals. For readers who are less focused on physique outcomes, the recommendation is essentially the same: build a movement habit that includes both aerobic and resistance components, and maintain a body composition that reflects a healthy adiposity range.
What About Alcohol?
Alcohol is a well-established risk factor for colorectal cancer, with no clearly established safe threshold. Risk scales with quantity consumed, and the association has been documented across large prospective studies with reasonable consistency.
The mechanism involves the metabolism of ethanol to acetaldehyde, which is a known carcinogen that damages DNA and interferes with DNA repair. Alcohol also affects the gut microbiome, increases intestinal permeability, and can reduce absorption of protective nutrients including folate.
The IARC classifies alcoholic beverages as a Group 1 carcinogen based on sufficient evidence for causation across several cancer types including colorectal. The magnitude of the effect at moderate intakes is smaller than for processed meat or for sustained low physical activity, but the direction of the association is consistent across studies.
Practical guidance in Australia and most other high-income countries has moved toward lower recommended intake thresholds over recent years. The Australian NHMRC guidelines recommend no more than 10 standard drinks per week and no more than four on any single day for adults, with the caveat that lower intakes reduce risk further and there is no established safe threshold for cancer risk.
For readers currently consuming alcohol at levels above these thresholds, moving toward the recommended range represents a meaningful and practically achievable adjustment. For readers consuming within the recommended range, reducing further would further reduce cancer risk but should be weighed against other considerations.
What Are the Practical Dietary and Lifestyle Habits That Support Risk Reduction?
The evidence on protective dietary and lifestyle habits for colorectal cancer risk reduction has been reasonably settled for years, even as population-level behaviour has drifted in the opposite direction. The practical framework combines habits to build with habits to reduce.
Habits to build:
Aim for a minimum of 25 to 30 grams of dietary fibre per day. This is achievable through a daily pattern that includes a serving of legumes (lentils, chickpeas, beans), a serving of whole grains (oats, brown rice, wholegrain bread), several servings of vegetables, and a serving or two of fruit with skin.
Include calcium sources regularly. Higher calcium intake is associated with modestly reduced colorectal cancer risk, likely through binding of bile acids in the colon. Practical sources include dairy products (milk, yoghurt, cheese), calcium-set tofu, and calcium-fortified plant milks.
Engage in regular physical activity, including both aerobic and resistance components. The Australian Physical Activity Guidelines recommend 150 to 300 minutes of moderate aerobic activity per week and muscle-strengthening activities on two or more days per week.
Maintain a healthy body composition. This does not require reaching a specific low body fat percentage, but rather sustaining a body composition that supports metabolic health across the long term.
Habits to reduce:
Limit processed meat consumption including bacon, deli meats, sausages, and ham. Processed meat is classified as a Group 1 carcinogen based on sufficient evidence for causation of colorectal cancer, and reducing intake is one of the more evidence-supported dietary adjustments available.
Keep unprocessed red meat in moderation. The World Cancer Research Fund suggests limiting intake to under 500 grams (cooked weight) per week, which corresponds to roughly three to four servings per week.
Limit alcohol consumption. There is no established safe threshold for colorectal cancer risk, and risk scales with quantity consumed. Moving toward the Australian NHMRC guidelines of no more than 10 standard drinks per week is a practical starting point for readers currently consuming above this range.
Wondering How to Actually Hold These Habits Together?
The evidence on protective habits for colorectal cancer risk reduction has been reasonably settled for years. What has moved is population behaviour, and that is where the harder work sits: knowing what to do is rarely the bottleneck. Holding a coherent pattern of fibre, food quality, body composition, and physical activity together across busy weeks and competing priorities is where nutrition support tends to matter most. Our team works with clients on the dietary and lifestyle patterns that support long-term health alongside their physique and training goals, matched to their individual context rather than a generic template.
When Should You Speak With a Doctor?
This article covers dietary and lifestyle factors that appear consistently across large prospective studies as protective against colorectal cancer risk. It does not cover diagnosis, screening decisions, or the management of specific symptoms, all of which are questions for a general practitioner or medical specialist.
Screening in Australia is available through the National Bowel Cancer Screening Program, which sends a free faecal immunochemical test (FIT) kit to eligible adults every two years. As of July 2024, the eligibility age was lowered to 45 (from 50 previously), and adults aged 45 to 49 can request a kit through the program. Adults with a family history of bowel cancer or specific hereditary syndromes may be eligible for earlier or more frequent screening, which is a discussion for a GP.
Symptoms that warrant a GP appointment regardless of age include persistent changes in bowel habits, blood in the stool, unexplained weight loss, persistent abdominal pain, or persistent fatigue. Younger adults presenting with these symptoms have historically been under-investigated relative to older adults, and the current recommendation is to seek assessment promptly rather than assume symptoms are benign.
Family history is a significant risk factor for colorectal cancer, and readers with a first-degree relative diagnosed with bowel cancer (particularly at a younger age) should discuss screening timing and frequency with their GP.
Practical Takeaways
Bowel cancer incidence has been rising in adults under 50 across high-income countries for two decades, with the sharpest rises in the 30 to 39 age group. In the US, colorectal cancer became the leading cause of cancer death in adults under 50 in 2023.
The exact cause of the rise remains unclear, but current evidence points to a combination of dietary and lifestyle changes (higher ultra-processed food intake, reduced physical activity, higher obesity rates, altered gut microbiome, sustained alcohol consumption) rather than a single identifiable factor.
Higher fibre intake is one of the most consistently supported protective factors, with each additional 10 grams per day associated with approximately 10 percent lower colorectal cancer risk. Most adults consume roughly half of the recommended 25 to 30 grams per day.
Processed meat is classified as a Group 1 carcinogen based on sufficient evidence for causation of colorectal cancer. Unprocessed red meat carries weaker evidence, with the WCRF suggesting a limit of approximately 500 grams cooked per week.
Body composition and physical activity operate as independent risk factors. Both aerobic and resistance training reduce risk, and maintaining a healthy body composition produces risk reduction beyond what dietary changes alone provide.
Screening in Australia is now available from age 45 through the National Bowel Cancer Screening Program. Symptoms including persistent changes in bowel habits, blood in the stool, unexplained weight loss, or persistent abdominal pain warrant a GP appointment regardless of age.
Frequently Asked Questions
Why is bowel cancer rising in young adults?
The exact cause remains unclear, but current evidence points to a combination of dietary and lifestyle changes that have compounded across generations. These include higher ultra-processed food consumption, reduced physical activity, higher rates of obesity, altered gut microbiome composition, and sustained alcohol consumption in younger cohorts. Most of the evidence is associational rather than causal, and the true mechanism likely involves several of these factors interacting rather than a single identifiable cause.
At what age should I start bowel cancer screening in Australia?
Australia's National Bowel Cancer Screening Program lowered the eligibility age to 45 in July 2024 (from 50 previously). Adults aged 45 to 49 can request a free faecal immunochemical test (FIT) kit through the program, and adults aged 50 to 74 are automatically mailed a kit every two years. Adults with a family history of bowel cancer or specific hereditary syndromes may benefit from earlier or more frequent screening, which is a discussion for a general practitioner.
Does fibre really reduce bowel cancer risk?
Yes, and it is one of the most consistently supported dietary protective factors in the research literature. A comprehensive meta-analysis of prospective studies found that each additional 10 grams of dietary fibre per day was associated with an approximately 10 percent reduction in colorectal cancer risk. The mechanism involves both the production of short-chain fatty acids (particularly butyrate) that support colonocyte health and reduced intestinal transit time that limits contact between the bowel wall and potential carcinogens.
Is processed meat really as harmful as smoking?
The Group 1 carcinogen classification for processed meat is often misinterpreted. IARC classifications describe the strength of evidence that something causes cancer, not the magnitude of the risk. Processed meat is in the same category as tobacco because the evidence for causation is strong, but the absolute increase in cancer risk from processed meat consumption is much smaller than from smoking. A daily 50-gram portion of processed meat is associated with approximately an 18 percent increase in colorectal cancer risk, which is meaningful but a different order of magnitude to the effects of tobacco.
Do I need to stop eating red meat entirely?
No. The evidence on unprocessed red meat is weaker and more contested than for processed meat. The World Cancer Research Fund suggests limiting unprocessed red meat to under 500 grams (cooked weight) per week, which corresponds to roughly three to four servings per week. Processed meat carries stronger evidence for a causal association and is where the most impactful reduction typically comes from.
Does exercise reduce bowel cancer risk independently of weight?
Yes. Meta-analyses of prospective studies have found that physically active individuals have approximately 20 to 25 percent lower colon cancer risk compared to sedentary individuals, with the protective effect observed independently of body mass index. The mechanisms include reduced intestinal transit time, improved insulin sensitivity, lower systemic inflammation, and effects on immune function. Both aerobic and resistance training contribute to the protective effect.
If you want help building the dietary and lifestyle patterns that support long-term health alongside your training and physique goals, our team can build a plan that fits your context, preferences, and constraints. You can enquire about coaching or book a consultation with our team.