Nearly half the global population has insufficient vitamin D levels, and the consequences extend well beyond bone health. A practical, evidence-stratified guide to what vitamin D does, who benefits most from supplementation, and how to get the dose right.
Vitamin D functions more like a steroid hormone than a traditional vitamin, influencing the expression of over 1,000 genes and playing roles in calcium absorption, bone mineralisation, muscle function, immune signalling, and mood regulation. Approximately 48% of the global population has serum vitamin D levels below 50 nmol/L, the threshold most commonly used to define insufficiency. The benefits of supplementation are most pronounced when correcting an existing deficiency, with strong evidence supporting improvements in bone mineral density and fracture risk, and context-dependent evidence for muscle strength, immune function, and falls risk reduction. Typical supplementation doses range from 1,000 to 4,000 IU of vitamin D3 daily, taken with a meal containing dietary fat to support absorption.
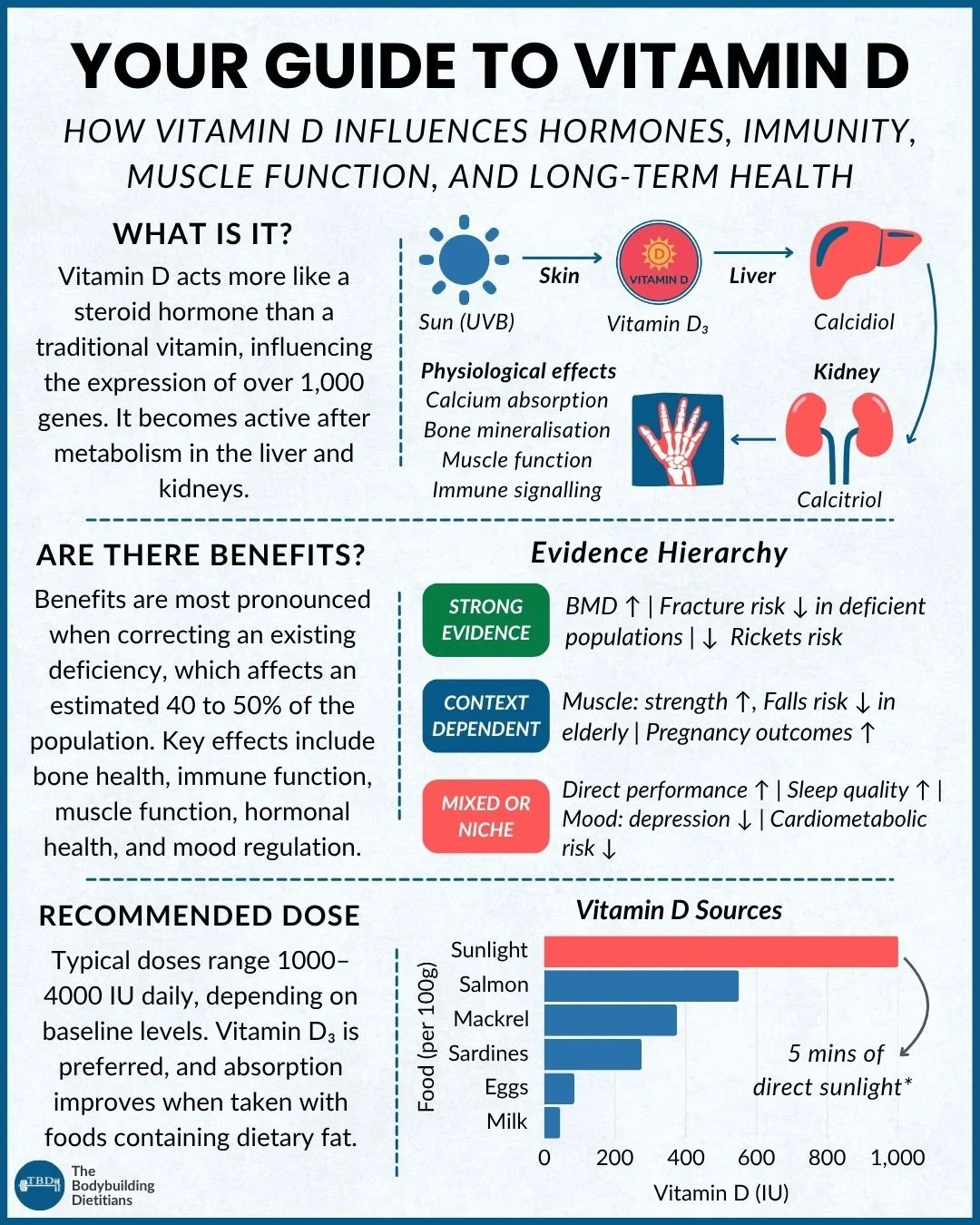
A visual guide to vitamin D covering its metabolic pathway, the evidence hierarchy for its benefits, recommended dosing, and the best dietary and environmental sources.
Vitamin D is one of the most common nutrient deficiencies globally, and the scope of its physiological influence is considerably broader than most people appreciate. While it is most commonly associated with bone health, vitamin D behaves less like a traditional vitamin and more like a steroid hormone, influencing the expression of over 1,000 genes across systems that include calcium metabolism, immune regulation, muscle function, hormonal health, and mood.
What makes this practically relevant is the scale of the deficiency problem. A pooled analysis of 7.9 million participants found that approximately 48% of the population has serum vitamin D levels below 50 nmol/L, the threshold most commonly used to define insufficiency. This means that roughly half of the general population may be experiencing the downstream consequences of inadequate vitamin D status without necessarily recognising it, because the symptoms of deficiency (fatigue, reduced immune resilience, impaired recovery, mood changes, and gradual bone density loss) develop slowly and are easily attributed to other causes.
A pooled analysis of global vitamin D status across 7.9 million participants from 81 countries found that approximately 47.9% of individuals had serum 25-hydroxyvitamin D levels below 50 nmol/L, with prevalence varying by latitude, season, skin pigmentation, and dietary habits. Deficiency rates were highest in regions with limited sunlight exposure and among populations with darker skin tones.
Source: Cashman et al., 2016, The Journal of Steroid Biochemistry and Molecular Biology.
The infographic above covers three key areas: what vitamin D is and how it works, the strength of evidence for its various benefits, and practical dosing guidance. The sections below expand on each one, with particular attention to how this applies to physically active individuals and those managing structured nutrition plans.
What Is Vitamin D and How Does It Work in the Body?
Vitamin D is a fat-soluble secosteroid that functions as a prohormone, requiring two metabolic conversions (in the liver and kidneys) before becoming biologically active. In its active form, it influences the expression of over 1,000 genes across multiple organ systems.
Vitamin D is synthesised in the skin when ultraviolet B (UVB) radiation from sunlight converts 7-dehydrocholesterol into cholecalciferol (vitamin D3). This inactive precursor is then transported to the liver, where it is converted to calcidiol (25-hydroxyvitamin D), the form measured in blood tests to assess vitamin D status. Calcidiol is subsequently converted in the kidneys to calcitriol (1,25-dihydroxyvitamin D), the biologically active form that binds to vitamin D receptors found throughout the body.
The reason vitamin D is often described as functioning more like a hormone than a vitamin is that its active form acts through a nuclear receptor (the vitamin D receptor, or VDR) that directly regulates gene transcription. Vitamin D receptors are present in virtually every tissue in the body, including bone, muscle, immune cells, the brain, the gut, and the pancreas. This widespread receptor distribution explains why the consequences of deficiency are not confined to a single system and why adequate vitamin D status has implications that extend well beyond the calcium and bone metabolism it is most commonly associated with.
The primary physiological effects of adequate vitamin D status include: enhanced calcium absorption in the gut (which is essential for bone mineralisation), regulation of phosphorus metabolism, support of skeletal muscle function and contractile capacity, modulation of both innate and adaptive immune responses, and influence on hormonal signalling pathways including testosterone production.
What Are the Benefits of Vitamin D and How Strong Is the Evidence?
The benefits of vitamin D are most pronounced when correcting an existing deficiency. The evidence base varies in strength across different outcomes, and understanding this hierarchy helps set realistic expectations about what supplementation can and cannot deliver.
The infographic organises the evidence into three tiers: strong, context-dependent, and mixed or niche. This stratification is important because the supplement industry often presents all potential benefits of a nutrient at the same level of certainty, which creates unrealistic expectations and makes it difficult for people to assess where the evidence is genuinely robust.
Strong Evidence
The strongest evidence for vitamin D supplementation relates to bone health. In populations with existing deficiency (serum levels below 50 nmol/L), correcting vitamin D status is consistently associated with increased bone mineral density, reduced fracture risk, and prevention of rickets in children. These effects are mediated primarily through vitamin D's role in calcium absorption: without adequate vitamin D, the body cannot absorb sufficient calcium from the diet to maintain bone mineralisation, regardless of how much calcium is consumed.
Bone mineral density (BMD) is a measure of the mineral content within a given volume of bone tissue. Higher BMD is associated with greater bone strength and reduced fracture risk. Vitamin D supports BMD by facilitating calcium absorption in the small intestine and regulating the balance between bone formation and resorption.
For physically active individuals, bone health may seem like a distant concern, but it becomes increasingly relevant over a competitive career, particularly for athletes who undergo repeated periods of energy restriction (which can independently impair bone density) and for female athletes at risk of relative energy deficiency in sport (REDs).
Context-Dependent Evidence
The evidence for vitamin D's effects on muscle strength, falls risk reduction in elderly populations, and pregnancy outcomes is positive but context-dependent, meaning the benefits are most clearly observed in specific populations or under specific conditions rather than universally.
For muscle function, the research suggests that correcting a deficiency can improve muscle strength and contractile capacity, particularly in older adults and individuals with baseline levels below 50 nmol/L. The mechanism is thought to involve vitamin D receptors in skeletal muscle tissue that influence calcium handling and protein synthesis within muscle fibres. For already-replete individuals, supplementation above sufficient levels does not appear to produce additional strength benefits.
A meta-analysis of randomised controlled trials examining vitamin D supplementation and muscle strength found that supplementation significantly improved muscle strength in individuals with baseline vitamin D levels below 30 nmol/L, with diminishing benefits at higher baseline levels. The effect was most pronounced in older adults and in lower limb strength.
Source: Beaudart et al., 2014, Journal of Clinical Endocrinology and Metabolism.
Mixed or Niche Evidence
The evidence for vitamin D's effects on direct athletic performance, sleep quality, depression, and cardiometabolic risk is more mixed. Some studies report positive associations, particularly in deficient populations, but the evidence is not yet consistent enough to make strong recommendations based on these outcomes alone.
For mood and depression, several observational studies have identified associations between low vitamin D status and increased depressive symptoms, and some interventional studies have reported improvements in mood following supplementation in deficient individuals. However, the effect sizes are modest and the research is complicated by the difficulty of separating vitamin D's independent effect from the broader lifestyle factors (sunlight exposure, outdoor activity, season) that correlate with both vitamin D status and mood.
For cardiometabolic risk, the evidence is similarly mixed. While observational data consistently associate low vitamin D levels with higher cardiovascular and metabolic disease risk, large-scale supplementation trials in replete populations have not produced the reductions in cardiovascular events that the observational data might have predicted. The current interpretation is that low vitamin D may be a marker of poor health rather than a direct cause, though correcting deficiency remains worthwhile for other well-established reasons.
What Is the Right Dose and How Should You Take It?
Typical supplementation doses range from 1,000 to 4,000 IU of vitamin D3 daily, depending on baseline levels, with absorption improved by taking the supplement alongside a meal containing dietary fat.
The appropriate dose depends substantially on the individual's starting point. Someone with serum levels well below 50 nmol/L may need higher initial doses (sometimes up to 4,000 IU daily or more for a loading period under clinical supervision) to correct the deficiency within a reasonable timeframe. Someone whose levels are close to or above the sufficiency threshold may maintain adequate status with a lower daily dose of 1,000 to 2,000 IU, or through a combination of sensible sun exposure and dietary intake.
Vitamin D3 (cholecalciferol) is the preferred supplemental form because it is more effective at raising and maintaining serum 25-hydroxyvitamin D levels than vitamin D2 (ergocalciferol). This distinction is worth knowing, because some supplements and fortified foods use D2, which is less potent and less sustained in its effect on blood levels.
A meta-analysis of 42 randomised controlled trials found that vitamin D3 supplementation of longer than three years was associated with a modest but statistically significant reduction in all-cause mortality, specifically in individuals with baseline levels below 50 nmol/L. Vitamin D3 supplementation was also consistently associated with an approximately 15% reduction in cancer mortality, an effect not replicated with vitamin D2.
Source: Zhang et al., 2019, BMJ.
A few practical details are worth highlighting:
Take it with dietary fat. Vitamin D is fat-soluble, which means it is absorbed more effectively when consumed alongside a meal that contains fat. Taking a vitamin D supplement on an empty stomach or with a fat-free meal significantly reduces absorption. Pairing it with breakfast or lunch that includes a source of dietary fat (eggs, avocado, nuts, olive oil, or similar) is a simple way to maximise uptake.
Consider vitamin K2 alongside D3. Vitamin K2 plays a complementary role by directing calcium toward bone tissue rather than allowing it to accumulate in soft tissue such as arterial walls. This becomes increasingly relevant at higher vitamin D supplementation doses, because vitamin D enhances calcium absorption, and without adequate K2, there is a theoretical risk of calcium being deposited in places other than bone. Many quality vitamin D supplements now include K2 for this reason.
Timing may matter. There is emerging evidence that taking vitamin D late in the evening may interfere with melatonin production and disrupt sleep onset. While this research is still developing and not yet definitive, taking the supplement earlier in the day (with breakfast or lunch) is a reasonable precaution that aligns with the fat-containing meal recommendation and avoids any potential sleep disruption.
Baseline testing is worthwhile. Because the appropriate dose varies considerably depending on starting levels, getting a blood test for serum 25-hydroxyvitamin D is worth doing where accessible. This provides a clear starting point, allows for a dose that is proportional to the actual deficiency, and enables follow-up testing to confirm that levels have reached the target range. In Australia, this test can be requested through a GP and is covered by Medicare in many clinical circumstances.
Where Does Vitamin D Come From?
Vitamin D is obtained through three pathways: synthesis in the skin from UVB sunlight exposure, dietary intake from a limited number of foods, and supplementation.
Sunlight is the most potent natural source of vitamin D. Approximately five minutes of direct sunlight on exposed skin (face, arms, and hands) during peak UV hours can produce roughly 1,000 IU of vitamin D, though this figure varies considerably depending on skin tone, latitude, season, time of day, cloud cover, and sunscreen use. Individuals with darker skin require more sun exposure to produce the same amount of vitamin D because melanin reduces UVB penetration.
In Australia, the balance between sufficient sun exposure for vitamin D synthesis and skin cancer prevention is a genuine consideration. During summer months in most of Australia, incidental sun exposure during daily activities is often sufficient to maintain adequate vitamin D levels. During winter, particularly in southern states, reduced UV intensity and shorter daylight hours make it substantially more difficult to maintain levels through sunlight alone, which is when supplementation becomes more practically important.
Dietary sources of vitamin D are limited. The richest food sources are oily fish (salmon, mackerel, and sardines), which provide meaningful amounts per serve, and eggs, which contribute a more modest amount. Milk and some other products are fortified with vitamin D in certain countries, though the amounts added through fortification are generally insufficient to correct a deficiency on their own. For most people, dietary intake alone does not provide enough vitamin D to maintain optimal levels, particularly during periods of limited sun exposure.
This is one of the reasons vitamin D is among the most commonly recommended supplements for the general population, and especially for physically active individuals who may have increased turnover through exercise, sweat, and the metabolic demands of training. For people following structured nutrition plans where food selection is driven primarily by macronutrient targets, dietary vitamin D intake tends to be even lower unless oily fish is consumed regularly.
Why Does Vitamin D Matter for Lifters and Physique-Focused Individuals?
Vitamin D is relevant for physically active individuals because of its roles in muscle function, recovery, immune resilience, bone health, and hormonal status, all of which directly influence the ability to train effectively and adapt over time.
Muscle function. Vitamin D receptors are present in skeletal muscle tissue, and adequate vitamin D status supports calcium handling within muscle fibres, neuromuscular signalling, and the contractile capacity of the muscle. Correcting a deficiency has been associated with improvements in muscle strength and power output, particularly in the lower limbs. For athletes, maintaining adequate levels provides a physiological foundation that supports training quality, while deficiency introduces a limitation that may not be immediately obvious but accumulates over time.
Immune resilience. Vitamin D plays a regulatory role in both innate and adaptive immune function. Deficiency is associated with increased susceptibility to upper respiratory tract infections, which are a common cause of missed training days. For athletes in demanding training blocks or competition preparation, where immune function is already under pressure from high training loads and energy restriction, maintaining adequate vitamin D status provides one additional layer of immune support.
Bone health. Repeated training cycles that include periods of energy restriction (fat loss phases, contest preparation) can place cumulative stress on bone density over time, particularly for female athletes. Adequate vitamin D status supports calcium absorption and bone mineralisation, which provides protection against the bone density losses that can occur during extended periods of low energy availability.
Hormonal status. Vitamin D plays a role in testosterone production, and observational studies have identified associations between low vitamin D levels and lower testosterone in men. While supplementation does not reliably increase testosterone in individuals with already-adequate levels, correcting a deficiency removes one potential contributor to suboptimal hormonal status, which is relevant for natural athletes whose capacity for muscle growth and recovery depends on maintaining their hormonal environment within its natural range.
If you are managing a structured training and nutrition plan and want to ensure that your micronutrient status (including vitamin D) is supporting rather than limiting your progress, a consultation with one of our dietitians can help you identify where practical adjustments to diet or supplementation may be beneficial.
How Does Energy Restriction Affect Vitamin D Status?
Extended periods of energy restriction, such as those involved in fat loss phases and contest preparation, can compromise vitamin D status through reduced dietary intake, decreased fat tissue storage, and the physiological stress of sustained calorie deficits.
Vitamin D is stored in adipose (fat) tissue, and as body fat decreases during a deficit, the available storage pool for vitamin D diminishes. Dietary intake of vitamin D may also decrease if the individual's food choices become more restricted, particularly if oily fish, eggs, and fortified foods are reduced in favour of leaner, lower-calorie options. The combined effect can result in a gradual decline in serum vitamin D levels across a prolonged deficit, which is often undetected because routine blood testing is not always part of the prep or fat loss process.
For competitors preparing for a show, where energy restriction is sustained for 16 to 24 weeks and body fat may reach very low levels, proactive vitamin D supplementation throughout the prep is a sensible baseline strategy. This is one of the areas where our bodybuilding coaching includes micronutrient considerations alongside macro targets, because the physiological demands of contest preparation extend well beyond calories and macronutrients into the broader nutritional environment that supports health, recovery, and performance.
Practical Takeaways
Vitamin D functions more like a steroid hormone than a traditional vitamin, influencing the expression of over 1,000 genes across systems including bone, muscle, immune function, and hormonal health.
Approximately 48% of the global population has vitamin D levels below the insufficiency threshold of 50 nmol/L. The benefits of supplementation are most meaningful when correcting an existing deficiency.
Typical supplementation doses range from 1,000 to 4,000 IU of vitamin D3 daily, depending on baseline levels. Vitamin D3 is preferred over D2 for its superior effect on serum levels and its association with reduced cancer mortality.
Take vitamin D with a meal containing dietary fat to maximise absorption, and consider taking it earlier in the day to avoid any potential interference with melatonin production and sleep onset.
Consider taking vitamin K2 alongside D3, particularly at higher doses, to support the direction of calcium toward bone rather than soft tissue.
Baseline blood testing for serum 25-hydroxyvitamin D is worthwhile where accessible, because the appropriate dose depends substantially on starting levels and a test provides a clear basis for individualised dosing.
Frequently Asked Questions
How much vitamin D should you take per day?
Typical supplementation doses range from 1,000 to 4,000 IU of vitamin D3 daily, depending on baseline serum levels, body size, and individual factors such as skin tone, latitude, and sun exposure habits. Individuals with confirmed deficiency (below 50 nmol/L) may benefit from higher initial doses to correct the deficiency within a reasonable timeframe, while those with adequate baseline levels may maintain status with 1,000 to 2,000 IU daily. Baseline blood testing is the most reliable way to determine an appropriate dose.
Should you take vitamin D3 or D2?
Vitamin D3 (cholecalciferol) is the preferred supplemental form because it is more effective at raising and maintaining serum 25-hydroxyvitamin D levels than vitamin D2 (ergocalciferol). Research has also found that vitamin D3, but not D2, is associated with a reduction in cancer mortality, which provides an additional reason to choose the D3 form. Most quality supplements use D3, but it is worth checking the label to confirm.
Does vitamin D help build muscle?
Vitamin D does not directly stimulate muscle growth in the way that protein or resistance training does, but adequate vitamin D status supports the physiological environment in which muscle function, recovery, and adaptation occur. Correcting a deficiency has been associated with improvements in muscle strength and contractile capacity, particularly in individuals with low baseline levels. For already-replete individuals, supplementation above sufficient levels does not appear to produce additional muscle-building benefits.
Can you get enough vitamin D from food alone?
For most people, dietary intake alone is insufficient to maintain optimal vitamin D levels, particularly during periods of limited sun exposure. The richest dietary sources are oily fish (salmon, mackerel, sardines) and eggs, but even regular consumption of these foods typically provides less than the 1,000 to 2,000 IU per day that many individuals need to maintain adequate serum levels. Supplementation is the most reliable strategy for ensuring sufficiency, particularly during winter months and for individuals who spend limited time outdoors.
When is the best time to take vitamin D?
Taking vitamin D with a meal that contains dietary fat (such as breakfast or lunch) maximises absorption, since vitamin D is fat-soluble and requires fat for effective uptake. There is also emerging evidence that taking vitamin D late in the evening may interfere with melatonin production and sleep onset, though this research is still developing. Taking the supplement earlier in the day with a fat-containing meal addresses both considerations.
Should you take vitamin K2 with vitamin D?
Taking vitamin K2 alongside vitamin D3 is a reasonable practice, particularly at higher supplementation doses. Vitamin K2 helps direct calcium toward bone tissue and away from soft tissue such as arterial walls, complementing the increased calcium absorption that vitamin D promotes. Many quality vitamin D supplements now include K2 for this reason, and the combination is considered safe and potentially beneficial for long-term bone and cardiovascular health.
If you would like to ensure that your supplementation and micronutrient strategy is supporting your training, recovery, and long-term health alongside your macronutrient targets, our team of qualified dietitians can help.