Visceral fat is metabolically active in ways that subcutaneous fat is not, and its health implications extend well beyond body composition. Understanding what drives its accumulation and what reduces it is relevant to anyone managing their long-term health.
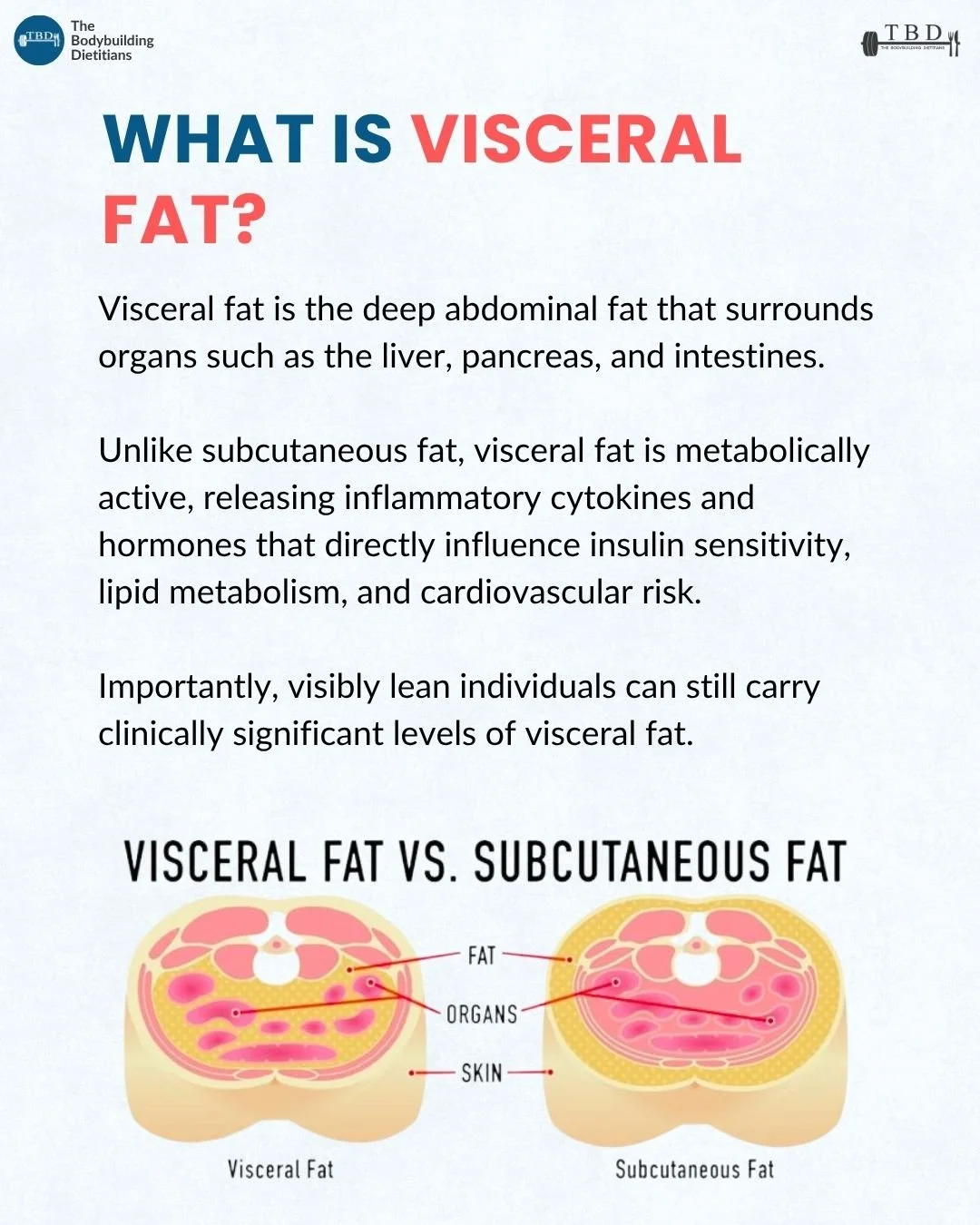
Visceral fat is the deep abdominal fat that surrounds internal organs including the liver, pancreas, and intestines. Unlike subcutaneous fat, which sits beneath the skin, visceral fat is metabolically active, releasing inflammatory cytokines and hormones that impair insulin sensitivity, alter lipid metabolism, and raise cardiovascular risk. Visibly lean individuals can carry clinically significant levels. The most effective strategies for reducing visceral fat combine a sustained calorie deficit with adequate protein and fibre intake, regular resistance and aerobic exercise, increased daily movement, improved sleep quality, reduced alcohol intake, and management of chronic stress. Even modest reductions in visceral fat tend to produce meaningful improvements in metabolic health markers before significant changes appear on the scale or in the mirror.

Body fat is not a uniform tissue. Where fat is stored, and what it does once it is there, matters considerably for health outcomes. Subcutaneous fat, the fat that sits beneath the skin and is visible and palpable, receives most of the attention in body composition discussions. Visceral fat, which sits deeper in the abdominal cavity surrounding vital organs, receives considerably less, despite carrying a more significant metabolic and cardiovascular risk profile.
The practical reality is that body weight and visible appearance are imperfect proxies for visceral fat. Individuals who appear lean can carry elevated visceral fat levels, and the health implications of that accumulation are real regardless of what the mirror or the scale shows. Understanding what visceral fat is, why it matters, and what actually moves the needle on reducing it is useful for anyone thinking seriously about their long-term health.
What Is Visceral Fat and How Does It Differ From Subcutaneous Fat?
Visceral fat is the adipose tissue stored deep within the abdominal cavity, surrounding organs including the liver, pancreas, and intestines. It differs from subcutaneous fat in both its location and its biological behaviour.
Subcutaneous fat sits beneath the skin and is the fat most people can see and pinch. While elevated subcutaneous fat contributes to body composition outcomes and carries its own health considerations at very high levels, it is comparatively metabolically inert. Visceral fat, by contrast, is metabolically active. It functions almost as an endocrine organ, releasing inflammatory cytokines, free fatty acids, and hormones that directly enter the portal circulation supplying the liver, creating effects on insulin sensitivity, lipid metabolism, and systemic inflammation that subcutaneous fat does not produce to the same degree.
One of the clinically important features of visceral fat is that its accumulation is not always visible from the outside. An individual can carry a clinically meaningful amount of visceral fat at a relatively normal body weight or with a body composition that appears lean by conventional standards. This is sometimes referred to as metabolically obese normal weight, a pattern in which visceral fat accumulation is present without the external appearance typically associated with elevated metabolic risk.
For this reason, body composition assessments that include visceral fat quantification, such as DEXA scanning, provide meaningfully more information than bodyweight or visual appearance alone.
Why Does Visceral Fat Affect Health Beyond Aesthetics?
The health risks associated with elevated visceral fat are well established and operate through several distinct mechanisms, all of which are linked to the metabolically active nature of the tissue.
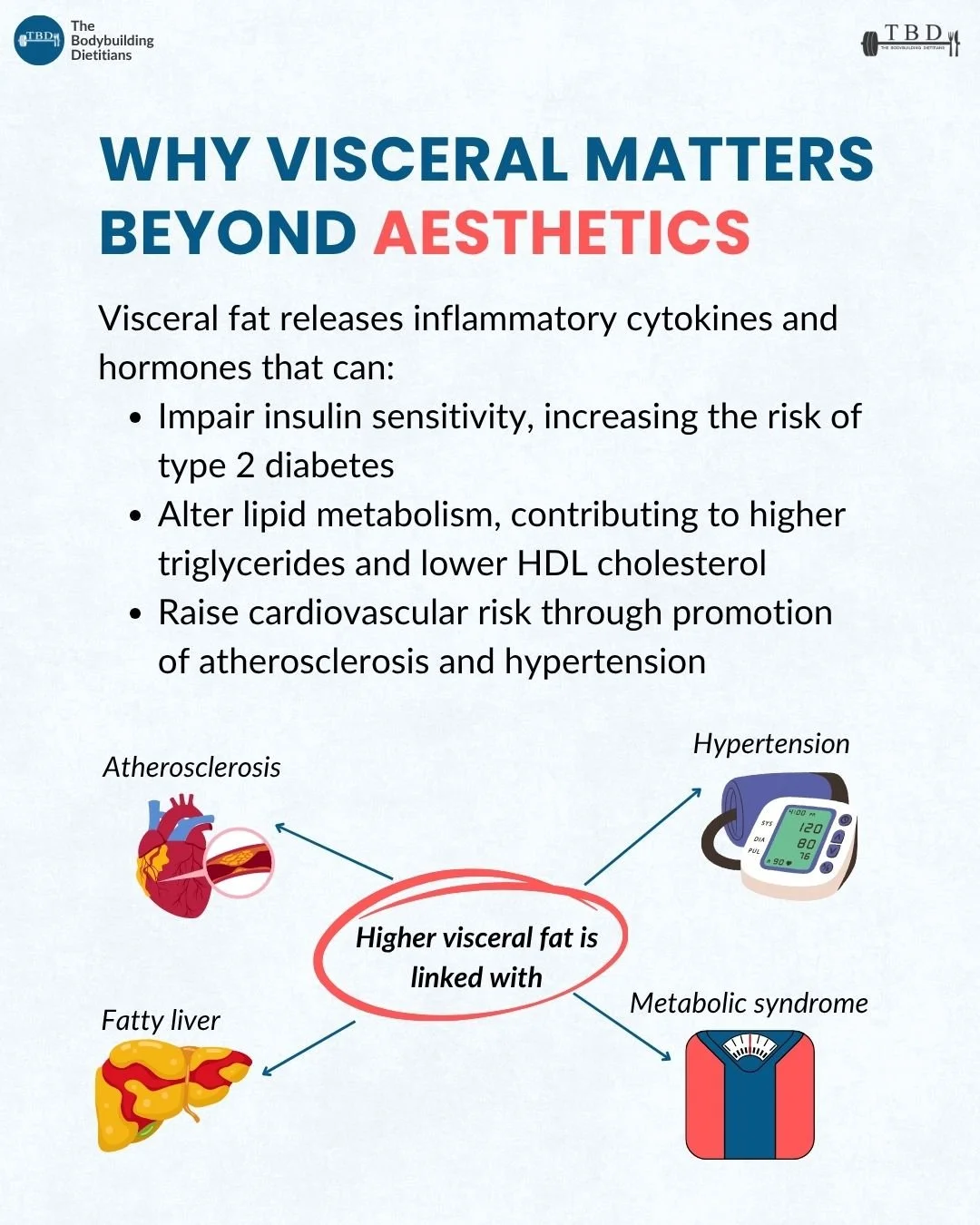
Visceral fat releases free fatty acids directly into the portal vein, which supplies the liver. This portal delivery of excess free fatty acids contributes to hepatic fat accumulation, impaired insulin clearance by the liver, and dysregulation of glucose production, all of which increase the risk of insulin resistance and, over time, type 2 diabetes.
The inflammatory cytokines released by visceral adipose tissue, including interleukin-6 and tumour necrosis factor alpha, contribute to a state of low-grade systemic inflammation. This chronic inflammatory environment is implicated in the development of atherosclerosis, the progressive narrowing and hardening of arterial walls that underpins much of cardiovascular disease risk.
Visceral fat also alters lipid metabolism in ways that are unfavourable for cardiovascular health. Higher visceral fat is consistently associated with elevated triglyceride concentrations and reduced HDL cholesterol, a lipid pattern associated with increased cardiovascular risk. Non-alcoholic fatty liver disease, which develops when excess fat accumulates in the liver tissue, is strongly linked to visceral adiposity and occurs across a wide range of body weights.
A large prospective study published in the New England Journal of Medicine found that abdominal adiposity, as measured by waist circumference, was independently associated with all-cause mortality even after adjusting for body mass index, with higher waist circumference associated with significantly elevated risk across both normal weight and overweight categories.
Source: Pischon et al., 2008, New England Journal of Medicine.
The practical implication is that reducing visceral fat has health consequences beyond changes in body composition. Even modest reductions tend to produce improvements in insulin sensitivity, lipid profiles, blood pressure, and inflammatory markers before significant changes appear on the scale or in the mirror.
What Nutritional Strategies Are Most Effective for Reducing Visceral Fat?
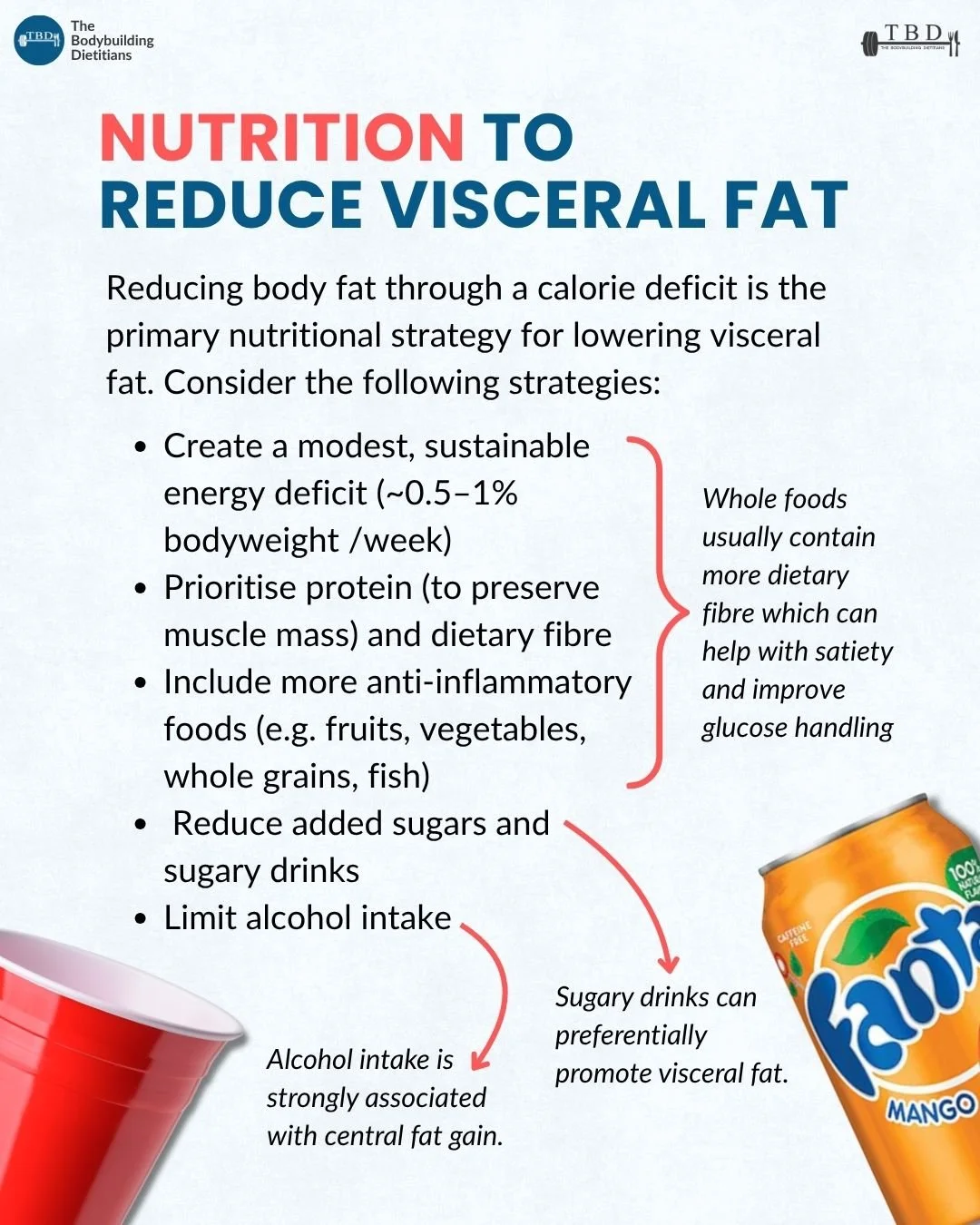
Reducing overall body fat through a sustained calorie deficit is the primary nutritional mechanism for lowering visceral fat. Visceral fat is generally responsive to energy deficit, and research consistently shows that it is mobilised during fat loss phases, often disproportionately relative to total fat mass, particularly in the early stages of a deficit.
A moderate, sustainable deficit of approximately 0.5 to 1 percent of bodyweight per week balances the rate of fat loss with the ability to maintain training performance, preserve muscle mass, and sustain adherence over time. More aggressive approaches may accelerate short-term weight loss but tend to compromise muscle retention, training quality, and long-term outcomes.
Adequate protein intake during a deficit is particularly important for preserving lean mass, which supports resting metabolic rate and long-term body composition. Dietary fibre plays a complementary role through its effects on satiety, glycaemic management, and gut health, all of which are relevant to the metabolic environment in which visceral fat accumulates. Whole foods, which tend to provide more fibre per calorie than processed alternatives, support these outcomes alongside the broader dietary pattern.
Reducing added sugar and sugary drinks is specifically worth noting in the context of visceral fat. Fructose, which is present in high concentrations in many sweetened beverages and processed foods, is preferentially metabolised in the liver and has been associated with greater visceral and hepatic fat accumulation compared to other carbohydrate sources.
Alcohol intake is strongly associated with central fat accumulation and is worth addressing explicitly. Alcohol contributes calories with minimal nutritional return, and its metabolic effects, including the prioritisation of alcohol metabolism over fat oxidation, and its association with increased energy intake and reduced dietary quality, make it a meaningful contributor to visceral fat in individuals who drink regularly.
A dietary pattern built around adequate protein, high fibre, anti-inflammatory whole foods including fruits, vegetables, whole grains, legumes, and fatty fish, reduced added sugar, and moderate or minimal alcohol covers the nutritional basis for reducing visceral fat effectively. This is also the dietary pattern that supports overall body composition goals and long-term metabolic health.
How Does Exercise Contribute to Visceral Fat Reduction?
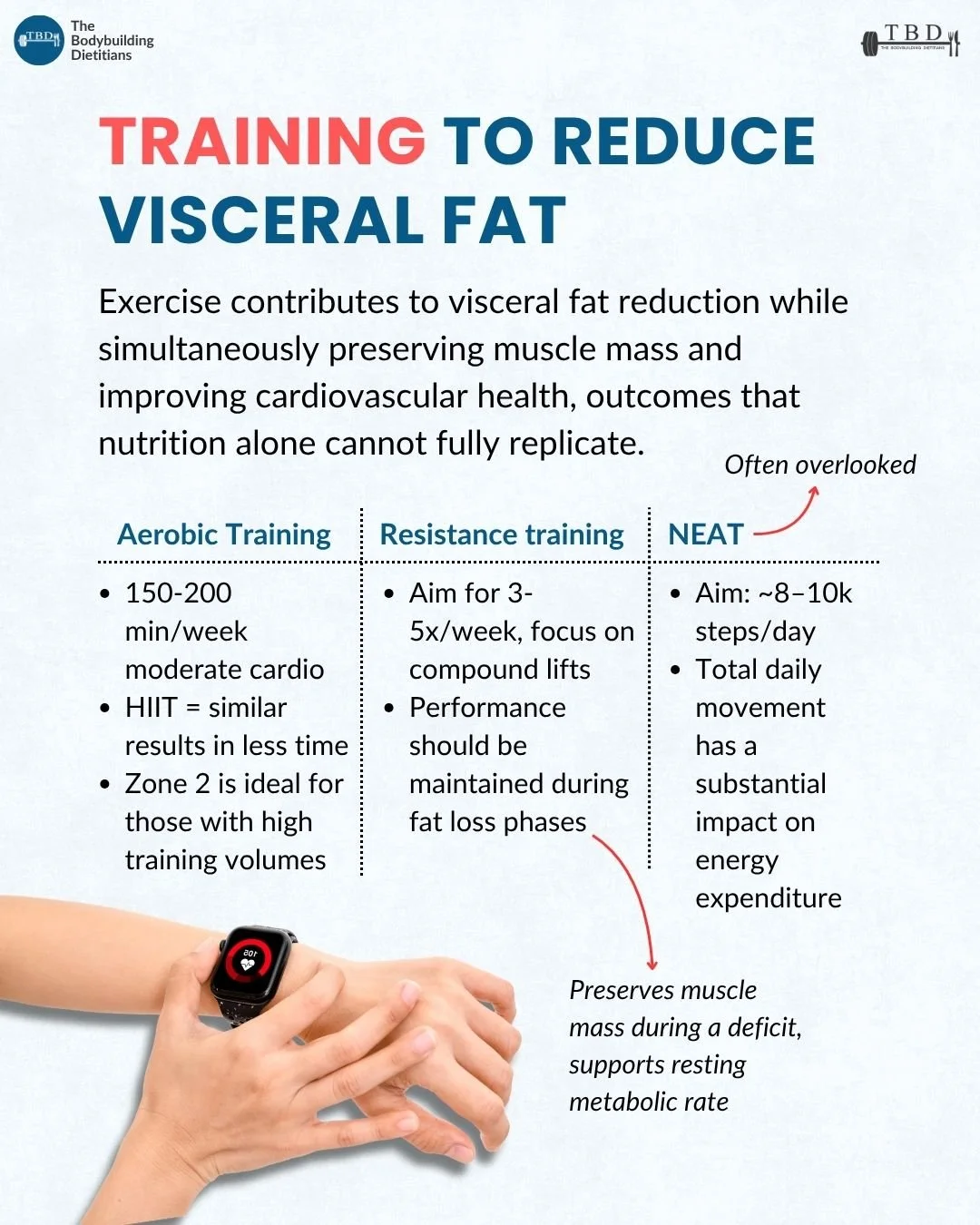
Exercise contributes to visceral fat reduction through multiple pathways: it increases energy expenditure, supports the calorie deficit that drives fat loss, preserves muscle mass during dieting, and improves insulin sensitivity and cardiovascular health independent of fat loss alone. These are outcomes that nutrition in isolation cannot fully replicate.
Aerobic training is well-supported for visceral fat reduction. Approximately 150 to 200 minutes per week of moderate-intensity cardio, such as brisk walking, cycling, or rowing, produces meaningful effects on visceral fat accumulation over time. High-intensity interval training produces comparable outcomes in less total training time and can be a practical option for individuals with higher training volumes or time constraints. Zone 2 training, which sits at a conversational aerobic intensity, is a useful modality for individuals already performing higher volumes of resistance training and who need additional cardiorespiratory work without accumulating excessive fatigue.
Resistance training contributes to visceral fat reduction both directly, through the energy expenditure it creates, and indirectly, by preserving the muscle mass that supports a higher resting metabolic rate during a deficit. Research suggests that resistance training alone can reduce visceral fat even without large changes in body weight, likely through improvements in insulin sensitivity and metabolic function. Maintaining training performance across a fat loss phase is an important indicator that the approach is sustainable and that muscle mass is being adequately protected.
Daily non-exercise movement, or NEAT, is a variable that is often overlooked in discussions of training for fat loss. Targeting 8,000 to 10,000 steps per day adds meaningfully to total energy expenditure without interfering with recovery from structured training. The cumulative effect of consistent daily movement on weekly energy balance is substantial and represents a practical lever that operates independently of gym sessions.
What Lifestyle Factors Drive Visceral Fat Accumulation?
Beyond nutrition and structured exercise, several lifestyle factors independently influence visceral fat accumulation, and addressing them is an important part of a comprehensive approach.
Chronic energy surplus is the most fundamental driver: consistently consuming more energy than is expended promotes fat storage across all depots, including visceral. Low physical activity compounds this by reducing total energy expenditure and impairing metabolic health independently of body weight, meaning that sedentary behaviour carries metabolic risk even in individuals who are not visibly overweight.
Sleep quality has a direct relationship with both appetite regulation and fat distribution. Poor sleep elevates ghrelin, suppresses leptin, increases cortisol, and impairs insulin sensitivity, all of which create conditions that promote fat storage and make dietary adherence more difficult. The relationship between sleep and body composition is meaningful enough to consider sleep a legitimate target variable in any approach to reducing visceral fat.
Chronic psychological stress elevates cortisol, which promotes abdominal fat storage, increases appetite for energy-dense foods, and disrupts sleep quality. The combination of elevated cortisol, disrupted sleep, and reduced dietary control creates a compounding environment that preferentially promotes visceral fat accumulation over time. Managing stress is therefore not tangential to fat loss or body composition management; it is part of the same system.
Excess alcohol intake is strongly associated with central fat gain, both through its direct caloric contribution and through its effects on liver metabolism, appetite, and food choice. Addressing alcohol intake is one of the most impactful single changes available to individuals with elevated visceral fat who drink regularly.
The lifestyle drivers of visceral fat are largely modifiable, and the good news from the research is that modest reductions in visceral fat, achieved through any combination of the strategies above, tend to produce improvements in metabolic markers, lipid profiles, and insulin sensitivity that become measurable well before large changes appear on the scale or in the mirror. This makes the early stages of a structured approach to reducing visceral fat particularly rewarding from a health standpoint, even when the aesthetic changes are still modest. For individuals who want professional support in building that structure, a consultation with one of our dietitians can help translate these principles into a plan that fits their specific situation.
Practical Takeaways
Visceral fat is the deep abdominal fat surrounding organs such as the liver, pancreas, and intestines. Unlike subcutaneous fat, it is metabolically active and releases inflammatory signals that directly affect insulin sensitivity, lipid metabolism, and cardiovascular risk.
Visibly lean individuals can carry clinically significant levels of visceral fat. Body weight and appearance are imperfect proxies for visceral adiposity.
A sustained calorie deficit, targeting approximately 0.5 to 1 percent of bodyweight loss per week, is the primary nutritional mechanism for reducing visceral fat. Adequate protein and dietary fibre intake supports muscle preservation and adherence during the process.
Reducing added sugar, sugary drinks, and alcohol intake addresses specific nutritional contributors to visceral and hepatic fat accumulation that go beyond total calorie balance.
A combination of aerobic training, resistance training, and consistent daily movement provides the most comprehensive exercise approach to visceral fat reduction, with benefits extending beyond those achievable through nutrition alone.
Sleep quality, chronic stress, and physical activity levels are lifestyle variables that independently influence visceral fat accumulation and are worth addressing alongside dietary changes.
Even modest reductions in visceral fat tend to produce measurable improvements in insulin sensitivity, lipid profiles, and blood pressure before significant changes appear on the scale or in the mirror.
Frequently Asked Questions
Can you have high visceral fat if you look lean?
Yes. Visceral fat accumulates in the deep abdominal cavity and is not always visible or palpable from the outside. Individuals who appear lean by conventional standards can still carry clinically significant levels of visceral fat, particularly if they are sedentary, have a history of poor dietary habits, or carry most of their fat internally rather than subcutaneously. Body composition assessments such as DEXA scanning that quantify visceral fat provide more accurate information than bodyweight or visual appearance alone.
How is visceral fat measured?
The most accurate methods for measuring visceral fat are DEXA scanning, which estimates visceral adipose tissue as part of a full body composition assessment, and abdominal CT or MRI scanning, which provides direct imaging of visceral fat volume. Waist circumference is a practical proxy that correlates reasonably well with visceral fat levels in clinical and population research, with values above 94 cm in males and 80 cm in females associated with elevated metabolic risk. Waist-to-hip ratio is an additional simple measure that provides useful information about central fat distribution.
Does spot reduction of abdominal fat work?
Spot reduction, the idea that exercising a specific area of the body preferentially reduces fat in that area, is not supported by evidence. Fat loss occurs systemically in response to an overall energy deficit, with the distribution of loss influenced more by genetics, hormones, and the degree of deficit than by which muscles are being trained. Abdominal exercises build and strengthen the underlying musculature but do not selectively reduce visceral or subcutaneous fat in that region.
Is visceral fat more dangerous than subcutaneous fat?
Visceral fat carries a greater metabolic and cardiovascular risk than subcutaneous fat at equivalent amounts, primarily because of its metabolic activity and its anatomical proximity to the portal circulation supplying the liver. The inflammatory cytokines, free fatty acids, and hormones released by visceral fat affect insulin sensitivity, lipid metabolism, and systemic inflammation in ways that subcutaneous fat does not to the same degree. This does not mean subcutaneous fat is without health implications at very high levels, but the risk profile of visceral fat is distinctly more significant.
How long does it take to reduce visceral fat?
Visceral fat tends to respond relatively quickly to a sustained energy deficit, with research showing measurable reductions in visceral fat mass within 8 to 12 weeks of a structured dietary and exercise intervention. The rate of reduction depends on the size of the energy deficit, total training volume, and the individual's starting point. Improvements in metabolic markers such as insulin sensitivity and triglycerides often appear within the first few weeks of a well-structured approach, even before large changes in body weight or appearance are visible.
Does alcohol increase visceral fat specifically?
Yes. Alcohol intake is consistently associated with central and visceral fat accumulation through several mechanisms. Alcohol is metabolised preferentially in the liver, which displaces fat oxidation and promotes hepatic fat storage. It contributes directly to calorie intake with no nutritional return, and it tends to increase appetite and reduce dietary quality. Heavy and regular alcohol intake is a meaningful driver of visceral and hepatic fat accumulation, and reducing intake is one of the more impactful single changes available to individuals with elevated visceral fat who drink regularly.
If you would like professional support in assessing your body composition and building a structured approach to reducing visceral fat, our team of dietitians can help.