Iron, vitamin D, magnesium, calcium, and iodine are the five nutrient gaps most consistently seen in active individuals. Understanding why they occur, what the symptoms look like, and how to address them through diet and targeted supplementation can meaningfully improve training, recovery, and long-term health.
The five most clinically relevant nutrient deficiencies for physically active individuals are iron (particularly in active females, affecting oxygen transport and endurance), vitamin D (affecting bone health, immune function, and muscle function, with approximately 48% of the global population insufficient), magnesium (involved in over 300 enzymatic reactions including muscle contraction and sleep), calcium (essential for bone mineral density and often low during energy restriction), and iodine (critical for thyroid function and commonly overlooked). Higher training demands, increased losses through sweat, structured diets that prioritise macronutrients over food diversity, and periods of energy restriction all raise the risk of these deficiencies. Baseline blood testing is the most reliable way to identify individual gaps and guide appropriate dietary or supplementation strategies.
Statistically, most people reading this are likely deficient in at least one of the nutrients covered in this article. That is not an alarmist claim. It is a reflection of what population-level data consistently shows when intake of these five micronutrients is measured against established adequacy thresholds.
The reasons vary from person to person, but several factors that are common among physically active individuals raise the risk of these deficiencies specifically. Higher training demands increase the turnover and loss of certain minerals through sweat and metabolic processes. Structured nutrition plans that prioritise protein and calorie targets over food diversity can inadvertently restrict the range of micronutrient-rich foods in the diet. Periods of energy restriction, which are a routine part of fat loss and contest preparation, reduce total food intake and with it the opportunity to meet micronutrient needs from diet alone.
The symptoms of these deficiencies tend to be non-specific: fatigue, disrupted sleep, flat training sessions, poor recovery, low mood, and increased susceptibility to illness. These are easy to attribute to training load, stress, or insufficient rest, which is part of why deficiencies can go unaddressed for longer than they should. Understanding which nutrients are most commonly insufficient, what the risk factors are, and how to address them through diet and targeted supplementation provides a practical framework for closing gaps that may be quietly undermining progress.
Iron: Why It Matters and Who Is Most at Risk
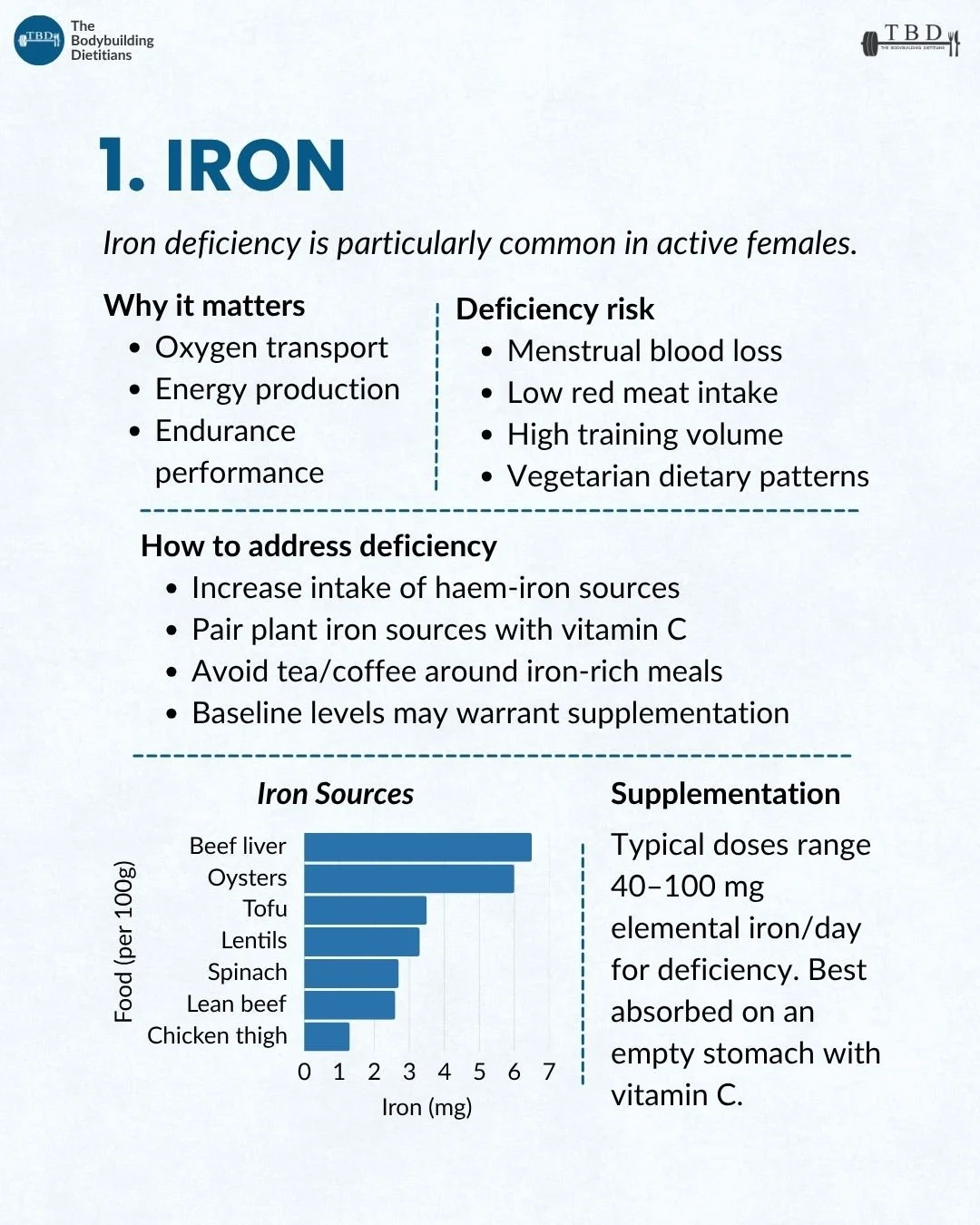
Iron deficiency is one of the most common nutrient deficiencies globally and is particularly prevalent among active females, vegetarians, and individuals with high training volumes.
Iron is an essential mineral that plays a central role in oxygen transport (as a component of haemoglobin in red blood cells), energy production (through its involvement in the electron transport chain), and endurance performance. Iron deficiency, even before it progresses to full anaemia, can manifest as unexplained fatigue, reduced exercise capacity, impaired recovery, and increased susceptibility to illness.
The populations most at risk of iron deficiency among active individuals include: females of menstruating age (due to regular iron losses through menstruation), individuals with low red meat intake (haem iron from animal sources is more bioavailable than non-haem iron from plant sources), athletes with high training volumes (exercise increases iron losses through sweat, gastrointestinal bleeding, and foot-strike haemolysis in runners), and those following vegetarian or vegan dietary patterns.
A systematic review of iron status in female athletes found that iron depletion (low ferritin stores) was present in approximately 15 to 35% of female athletes across various sports, with higher prevalence in endurance sports and among those with restricted energy intake. The review noted that even subclinical iron deficiency (depleted stores without anaemia) was associated with reduced aerobic capacity and impaired training adaptation.
Source: Sim et al., 2019, Nutrients.
How to address iron through diet. The most bioavailable dietary iron comes from haem sources: red meat, liver, oysters, and other animal proteins. Including haem iron sources regularly (three to four serves of red meat per week, for example) is one of the most effective dietary strategies for maintaining iron status. For plant-based iron sources (lentils, tofu, spinach, fortified cereals), pairing them with a source of vitamin C (citrus, capsicum, tomato) at the same meal significantly enhances absorption. Avoiding tea and coffee in the hour surrounding iron-rich meals is also worthwhile, as the tannins and polyphenols in these beverages can reduce non-haem iron absorption by up to 60%.
When to consider supplementation. Iron supplementation should be guided by blood testing (serum ferritin and full blood count) rather than taken presumptively, because excess iron intake carries its own health risks. When deficiency is confirmed, typical supplementation doses range from 40 to 100 mg of elemental iron per day, best absorbed on an empty stomach with vitamin C. Some individuals tolerate iron better when taken with a small amount of food, and alternate-day dosing has been shown to improve absorption efficiency in some studies.
Vitamin D: Why It Matters and Who Is Most at Risk
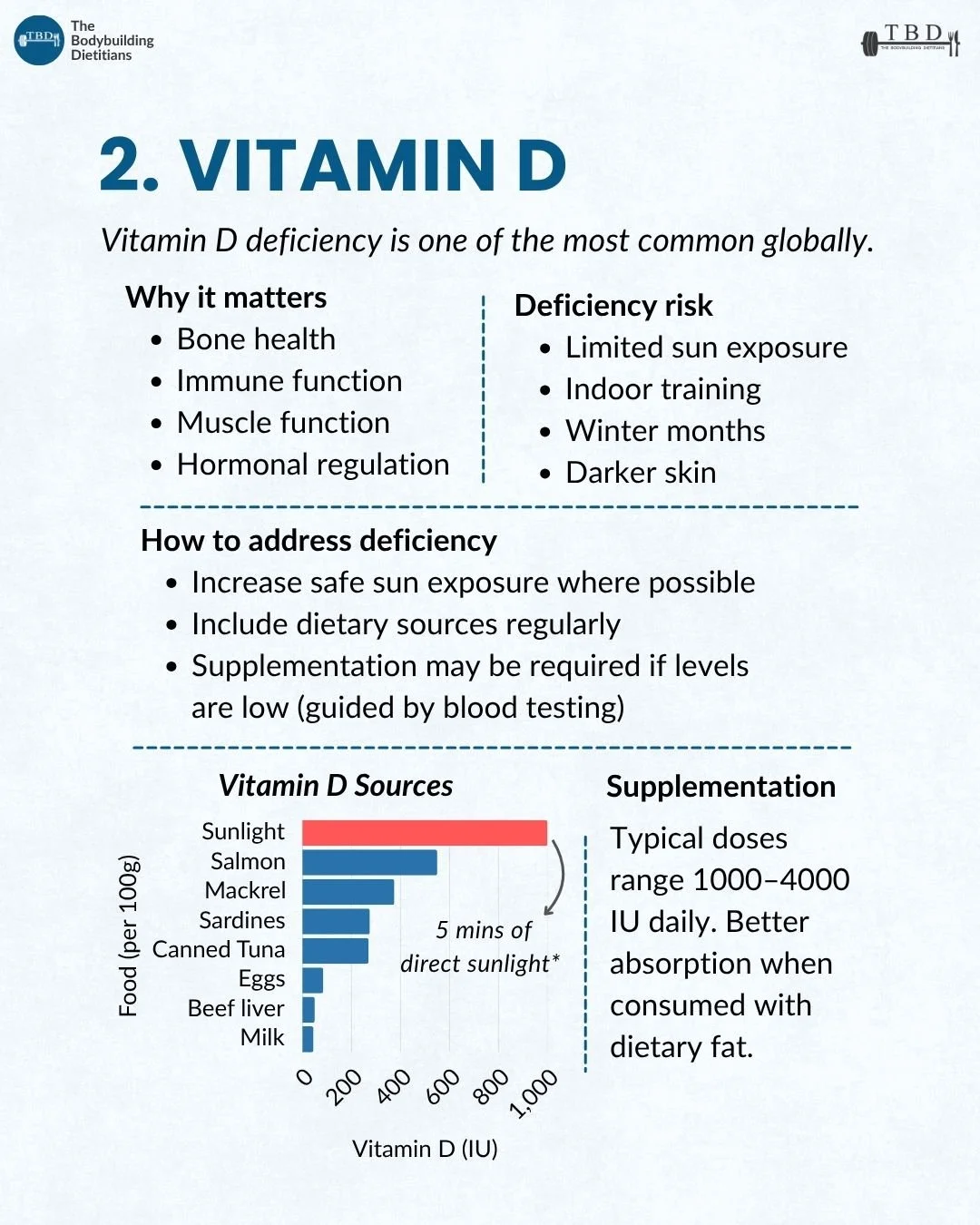
Vitamin D deficiency is one of the most common globally, affecting an estimated 48% of the population, and is particularly relevant for active individuals because of its roles in bone health, immune function, muscle function, and hormonal regulation.
Vitamin D functions more like a steroid hormone than a traditional vitamin, influencing the expression of over 1,000 genes after undergoing metabolic conversion in the liver and kidneys to its active form, calcitriol. The benefits of supplementation are most pronounced when correcting an existing deficiency, with strong evidence for improvements in bone mineral density and fracture risk, and context-dependent evidence for muscle strength and immune function.
The populations most at risk include individuals with limited sun exposure (indoor workers, those who train predominantly indoors), people in southern latitudes during winter months (including most of southern Australia from May to September), individuals with darker skin tones, and anyone undergoing extended periods of energy restriction where dietary intake of vitamin D sources may be reduced.
How to address it. Supplementation with 1,000 to 4,000 IU of vitamin D3 daily (taken with a meal containing dietary fat) is the most practical strategy for most people. Baseline blood testing for serum 25-hydroxyvitamin D provides the clearest basis for determining the appropriate dose. Dietary sources (oily fish, eggs, fortified milk) contribute but are generally insufficient on their own to maintain adequate levels.
Magnesium: Why It Matters and Who Is Most at Risk
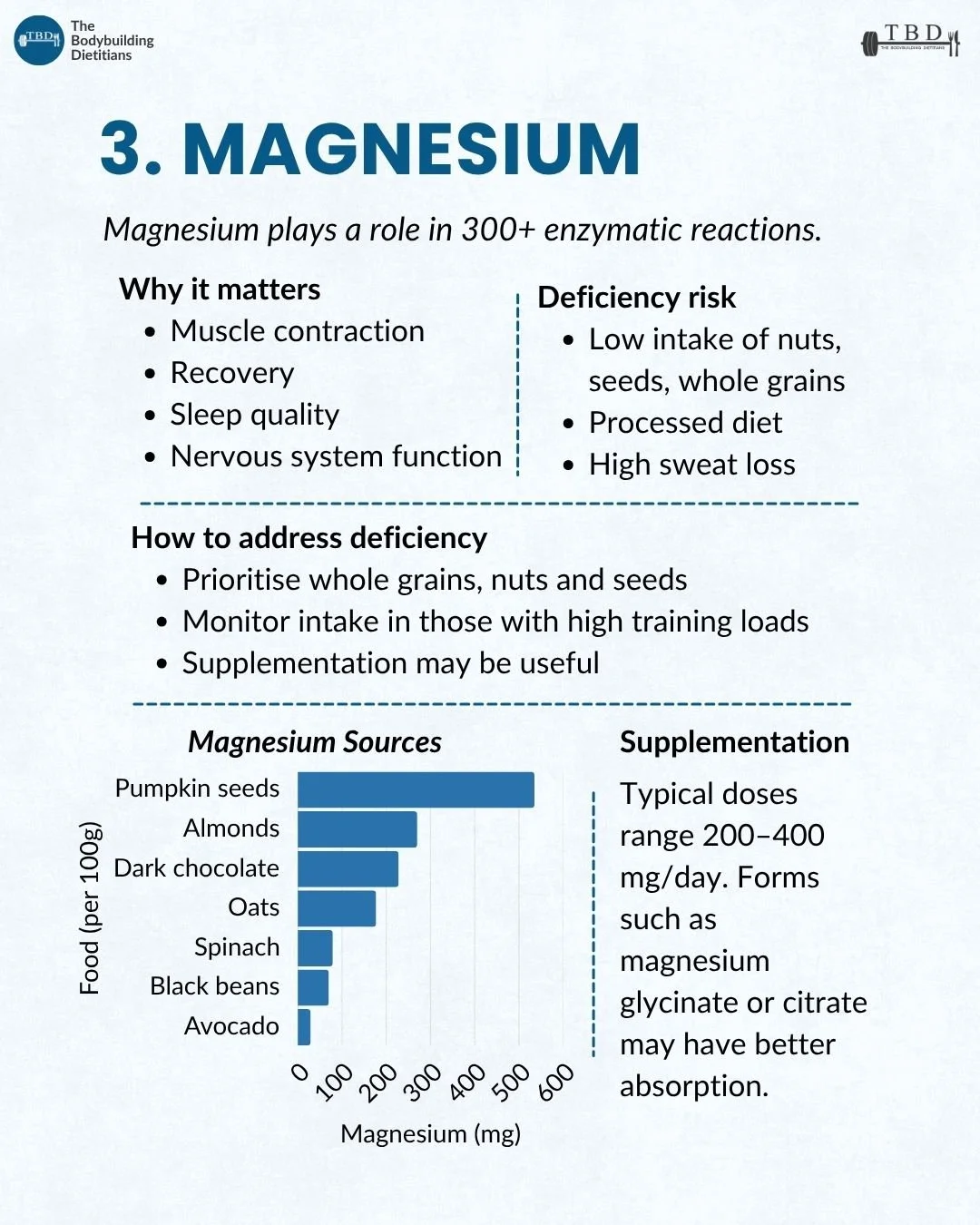
Magnesium is involved in over 300 enzymatic reactions in the body and plays essential roles in muscle contraction, recovery, sleep quality, and nervous system function. Subclinical deficiency is common and often undetected.
Magnesium is the fourth most abundant mineral in the body and a cofactor for enzymes involved in energy production (ATP synthesis), protein synthesis, muscle and nerve function, blood glucose regulation, and bone development. Magnesium also plays a direct role in sleep quality through its influence on the parasympathetic nervous system and its interaction with GABA receptors, which is part of why magnesium supplementation is frequently recommended for sleep support.
The populations most at risk of magnesium deficiency among active individuals include those with low intake of nuts, seeds, and whole grains (the richest dietary sources), individuals following highly processed or restrictive diets, and athletes with high training loads who lose magnesium through sweat. Magnesium losses through sweat can be meaningful during prolonged or intense training sessions, particularly in warm environments.
Research on magnesium status in athletes has found that a significant proportion of physically active individuals consume less than the estimated average requirement for magnesium, and that exercise itself increases magnesium requirements by 10 to 20% due to increased urinary and sweat losses. Subclinical magnesium deficiency has been associated with impaired exercise performance, increased oxygen consumption during submaximal exercise, and elevated inflammatory markers.
Source: Nielsen and Lukaski, 2006, Magnesium Research.
The best dietary sources of magnesium include pumpkin seeds (one of the most concentrated food sources), almonds, dark chocolate, oats, spinach, black beans, and avocado. Including a daily serve of nuts or seeds and prioritising whole grain carbohydrate sources over refined alternatives provides a strong foundation for dietary magnesium intake.
When to consider supplementation. Typical supplementation doses range from 200 to 400 mg per day. The form of magnesium matters for absorption and tolerability: magnesium glycinate is well-absorbed and less likely to cause gastrointestinal side effects than cheaper forms like magnesium oxide, and it is often preferred for sleep support due to the calming properties of the glycine component. Magnesium citrate is also well-absorbed and can support bowel regularity, which may be an additional benefit for some individuals. Taking magnesium in the evening aligns with its sleep-supporting effects and is a common practical recommendation.
Calcium: Why It Matters and Who Is Most at Risk
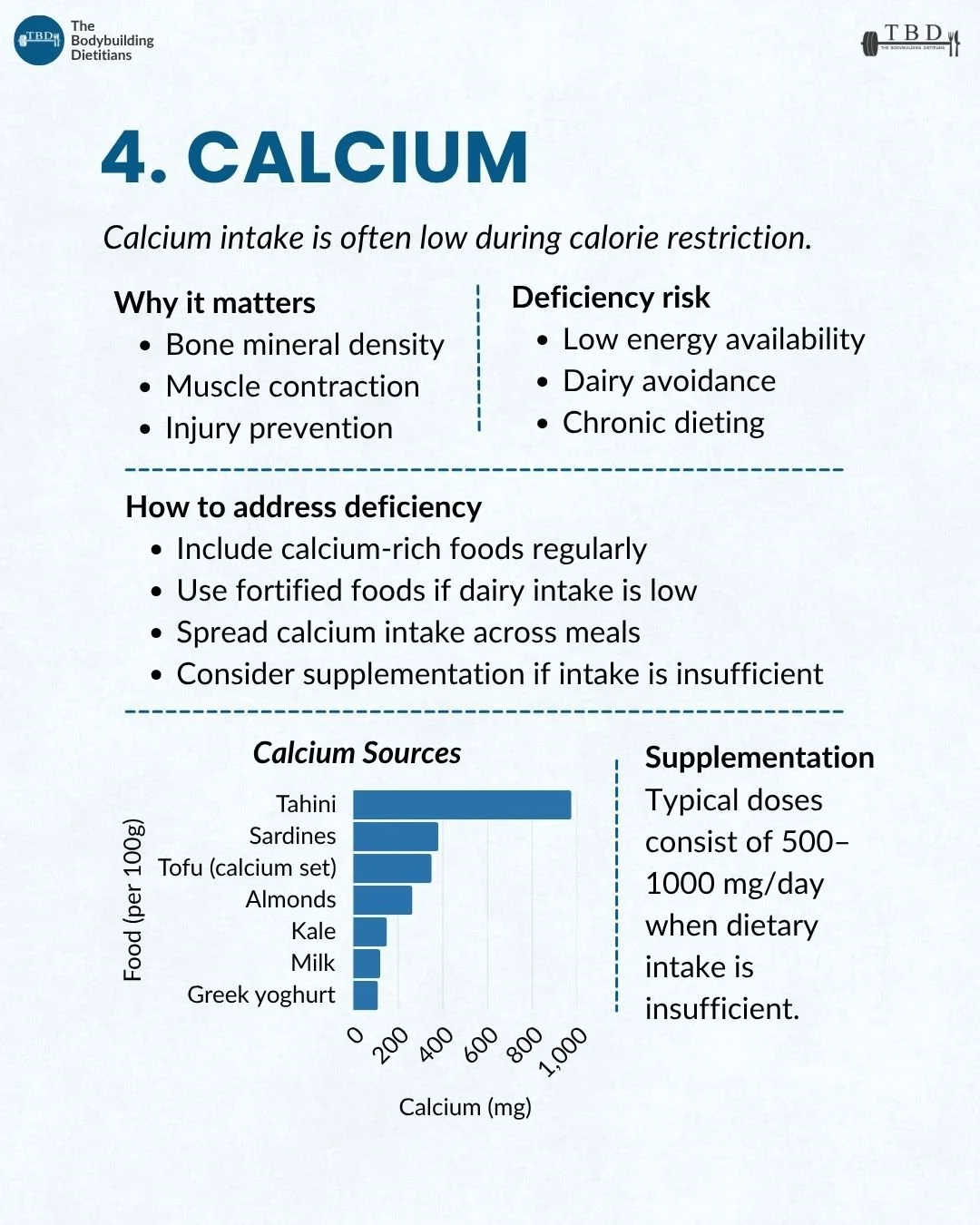
Calcium is the most abundant mineral in the body and is essential for bone mineral density, muscle contraction, and injury prevention. Intake is often low during periods of energy restriction, dairy avoidance, and chronic dieting.
Calcium is required for the structural integrity of bone and teeth (which contain approximately 99% of the body's calcium), and it plays critical roles in muscle contraction, nerve signalling, blood clotting, and intracellular signalling. When dietary calcium intake is insufficient, the body draws calcium from bone stores to maintain blood calcium levels, which over time contributes to reduced bone mineral density and increased fracture risk.
Bone mineral density (BMD) is a measure of the mineral content within a given volume of bone tissue. For physically active individuals, particularly those who undergo repeated cycles of energy restriction (fat loss phases, contest preparation), cumulative calcium insufficiency can contribute to progressive bone density loss that may not become clinically apparent until later in life.
The populations most at risk include individuals with low energy availability (anyone in a calorie deficit, particularly a prolonged or aggressive one), those who avoid or restrict dairy (which is the most concentrated and bioavailable dietary calcium source in most Western diets), and chronic dieters who have spent extended periods with below-maintenance calorie intake across multiple years.
The best dietary sources include dairy products (milk, yoghurt, cheese), calcium-set tofu, sardines (with bones), tahini, almonds, and kale. For individuals who consume dairy regularly, meeting calcium targets (approximately 1,000 mg per day for most adults) is relatively straightforward. For those who avoid or limit dairy, deliberate inclusion of calcium-rich alternatives and potentially fortified foods becomes important.
Practical strategies. Spreading calcium intake across multiple meals rather than concentrating it in a single serve supports more consistent absorption, because the body absorbs calcium most efficiently in doses of approximately 500 mg or less at a time. Including a calcium source at two to three meals per day provides a more effective absorption pattern than consuming the full daily target in one sitting.
When to consider supplementation. If dietary calcium intake consistently falls below the recommended 1,000 mg per day (which is common during energy restriction, particularly when dairy is limited), supplementation of 500 to 1,000 mg per day can help bridge the gap. Calcium supplements are best taken with food and, where possible, alongside vitamin D, which enhances calcium absorption.
Iodine: Why It Matters and Who Is Most at Risk
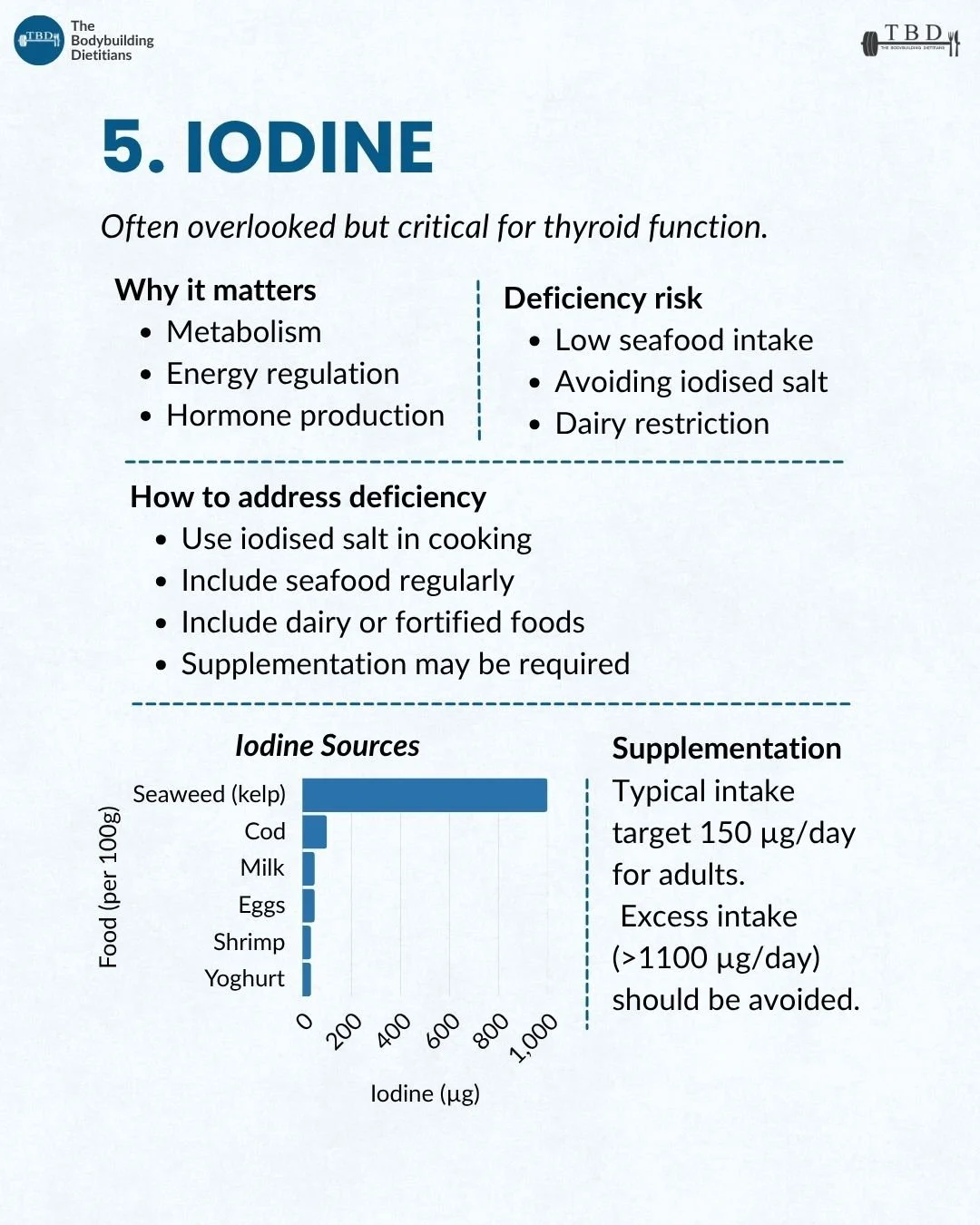
Iodine is often the most overlooked of the five nutrients covered here, but it is critical for thyroid function, which directly influences metabolism, energy regulation, and hormone production.
Iodine is an essential trace element required for the synthesis of thyroid hormones (T3 and T4), which regulate metabolic rate, energy production, growth, and development. Even mild iodine insufficiency can impair thyroid function, leading to symptoms including fatigue, weight gain, cold intolerance, dry skin, and cognitive sluggishness, all of which can be easily attributed to other causes and therefore go unrecognised.
Thyroid hormones (triiodothyronine, or T3, and thyroxine, or T4) are produced by the thyroid gland and regulate the rate of metabolic processes throughout the body. Adequate iodine intake is the primary dietary requirement for maintaining normal thyroid hormone production.
The populations most at risk include individuals with low seafood intake, those who use non-iodised salt (including sea salt and Himalayan salt, which typically contain little to no iodine), and people who restrict dairy products. In Australia, mandatory iodine fortification of bread flour (introduced in 2009) has improved population iodine status, but gaps remain, particularly among individuals who limit bread and dairy intake, which is common in physique-focused dietary patterns.
The best dietary sources include seaweed (kelp is an extremely concentrated source), seafood (cod, shrimp, canned tuna), dairy products (milk, yoghurt), and eggs. Using iodised salt in cooking is one of the simplest and most effective strategies for maintaining adequate iodine intake, and it is worth ensuring that the salt you use at home is iodised rather than a non-iodised alternative.
When to consider supplementation. The recommended daily intake for adults is approximately 150 micrograms per day. Most quality multivitamins include iodine at or near this level. Excessive iodine intake (above 1,100 micrograms per day) should be avoided, as it can paradoxically impair thyroid function, which is why concentrated kelp supplements require caution and should not be taken without professional guidance.
Why Are Active Individuals at Greater Risk of These Deficiencies?
The combination of higher physiological demands from training, structured diets that prioritise macronutrients over food diversity, and periods of energy restriction creates a set of conditions that systematically increase the risk of micronutrient gaps.
Training increases the demand for and turnover of several micronutrients. Iron is lost through sweat, gastrointestinal bleeding, and foot-strike haemolysis. Magnesium is lost through sweat and has increased demand due to its role in energy metabolism and muscle function. Calcium turnover increases with training load and bone remodelling. Vitamin D requirements may be higher in active individuals due to its roles in muscle function and immune regulation.
Structured nutrition plans, while effective for managing macronutrient targets, can inadvertently narrow the range of foods consumed. When protein and calorie targets dominate food selection, the foods that are richest in iron, magnesium, calcium, and iodine (red meat, shellfish, dairy, nuts, seeds, whole grains, and leafy green vegetables) may be underrepresented if they are not deliberately included.
Energy restriction compounds the problem by reducing total food intake, which proportionally reduces the opportunity to meet micronutrient needs from diet alone. This is why the later stages of a fat loss phase or contest preparation represent a particularly high-risk period for micronutrient inadequacy, and why proactive attention to food quality and, where necessary, targeted supplementation becomes progressively more important as calories decrease.
This is one of the areas where our coaching approach considers micronutrient adequacy alongside macro targets, because a diet that hits its protein, carbohydrate, and fat targets while falling short on iron, vitamin D, magnesium, calcium, and iodine is not a complete nutrition plan, regardless of how well the macros are structured.
Should You Get Blood Work Done?
Baseline blood testing is the most reliable way to understand where your individual gaps are and to guide supplementation decisions with precision rather than guesswork.
The symptoms of micronutrient deficiency are non-specific and overlap with many other causes of fatigue, poor recovery, and flat performance. Without blood testing, it is difficult to distinguish between iron deficiency, vitamin D insufficiency, poor sleep, overtraining, and the normal fatigue of a calorie deficit. Testing provides objective data that allows targeted intervention rather than a blanket approach of supplementing everything and hoping for the best.
The most relevant tests for active individuals include serum ferritin (iron stores), full blood count (to assess for anaemia), serum 25-hydroxyvitamin D (vitamin D status), and, where clinically indicated, serum magnesium, calcium, and thyroid function panels. In Australia, many of these tests can be requested through a GP and may be covered by Medicare depending on clinical indication.
A practical approach is to get baseline testing done at the start of a structured training or nutrition phase, particularly before entering a calorie deficit or contest preparation, and to repeat relevant tests periodically to monitor status over time. This allows supplementation to be adjusted based on actual need rather than assumed deficiency, which is both more effective and more cost-efficient.
If you would like professional guidance on which tests to request and how to interpret and act on the results within the context of your training and nutrition goals, a consultation with one of our dietitians can provide a structured starting point.
Practical Takeaways
Iron, vitamin D, magnesium, calcium, and iodine are the five nutrient deficiencies most consistently observed in active individuals. Most people are likely insufficient in at least one.
The symptoms of deficiency (fatigue, poor recovery, disrupted sleep, flat training sessions) are non-specific and easily attributed to other causes, which is why deficiencies often go unaddressed.
Iron deficiency is particularly common in active females and vegetarians. Prioritise haem iron sources, pair plant iron with vitamin C, and get ferritin levels tested before supplementing.
Vitamin D insufficiency affects approximately 48% of the global population. Supplementation with 1,000 to 4,000 IU of D3 daily (with dietary fat) is the most practical strategy for most people.
Magnesium supports muscle function, recovery, and sleep. Include nuts, seeds, and whole grains regularly, and consider magnesium glycinate supplementation (200 to 400 mg) in the evening if intake is low.
Calcium intake is often low during energy restriction and dairy avoidance. Spread calcium-rich foods across meals and consider supplementation if dietary intake consistently falls below 1,000 mg per day.
Iodine is critical for thyroid function and commonly overlooked. Use iodised salt, include seafood and dairy regularly, and check that your multivitamin includes iodine if dietary sources are limited.
Baseline blood testing is the most reliable way to identify individual gaps and guide targeted supplementation.
Frequently Asked Questions
What is the most common nutrient deficiency in athletes?
Iron and vitamin D are the two most prevalent nutrient deficiencies in physically active populations. Iron deficiency is particularly common among female athletes (affecting an estimated 15 to 35%) due to menstrual losses combined with increased exercise-related iron turnover. Vitamin D insufficiency affects approximately 48% of the general population and is even more prevalent among indoor athletes and those in higher latitudes during winter months.
Should athletes take a multivitamin?
A quality multivitamin can serve as a practical safety net for covering minor dietary gaps, but it should not replace a well-constructed diet that includes a variety of nutrient-dense whole foods. For active individuals, targeted supplementation based on blood testing (iron, vitamin D, magnesium) tends to be more effective than a blanket multivitamin approach, because the doses in most multivitamins are often insufficient to correct confirmed deficiencies. A multivitamin can complement targeted supplementation by covering nutrients like iodine, zinc, and B vitamins that may not warrant individual testing.
How do you know if you are iron deficient?
The most reliable way to assess iron status is through blood testing for serum ferritin (which reflects iron stores) and a full blood count (which can identify anaemia). Symptoms of iron deficiency include unexplained fatigue, reduced exercise capacity, shortness of breath during exertion, and increased susceptibility to illness, but these symptoms are non-specific and overlap with many other conditions. Blood testing provides objective confirmation and guides the appropriate supplementation dose.
Can you get enough magnesium from food?
Meeting magnesium requirements from diet alone is possible but requires deliberate inclusion of magnesium-rich foods, particularly nuts (almonds), seeds (pumpkin seeds), whole grains (oats), dark chocolate, and leafy greens. Active individuals with high training loads may have requirements 10 to 20% above the general population due to increased sweat and urinary losses, which can make dietary adequacy more challenging. If dietary intake is consistently below the recommended 400 mg per day for men or 310 mg for women, supplementation with 200 to 400 mg of a well-absorbed form (glycinate or citrate) is a practical strategy.
Is dairy the only good source of calcium?
Dairy products (milk, yoghurt, cheese) are the most concentrated and bioavailable dietary calcium sources, but they are not the only option. Calcium-set tofu, sardines with bones, tahini, almonds, and kale all provide meaningful calcium, and many plant milks are fortified to provide calcium levels comparable to dairy milk. For individuals who avoid dairy, deliberate inclusion of these alternatives and potentially supplementation is important to ensure adequate intake, particularly during phases of energy restriction where total food volume is reduced.
Why is iodine important for metabolism?
Iodine is required for the production of thyroid hormones T3 and T4, which regulate the rate of metabolic processes throughout the body. Insufficient iodine intake impairs thyroid hormone production, which can lead to a slower metabolic rate, fatigue, weight gain, and reduced energy levels. For active individuals managing body composition, adequate iodine intake supports the metabolic rate that underpins energy expenditure and fat loss, making it a practically relevant but often overlooked nutrient.
If you would like professional guidance on identifying and addressing nutrient gaps within your training and nutrition plan, our team of qualified dietitians can help.