Most supplements are not worth your money. Omega-3, vitamin D3, creatine monohydrate, and magnesium glycinate are the exceptions, each addressing a gap that diet alone reliably fails to close and each backed by a substantial body of evidence.
The four supplements with the strongest evidence base for physically active individuals are omega-3 fatty acids (2 to 3 grams of combined EPA and DHA daily for cardiovascular health, inflammation regulation, and brain function), vitamin D3 (approximately 2,000 IU daily for bone density, immune function, muscle function, and hormonal health), creatine monohydrate (3 to 5 grams daily for strength, power, muscle mass, and training performance), and magnesium glycinate (200 to 400 mg daily for sleep quality, muscle recovery, and nervous system function). Each of these addresses a common dietary insufficiency and has consistent, high-quality evidence supporting its use, which distinguishes them from the vast majority of supplements on the market.
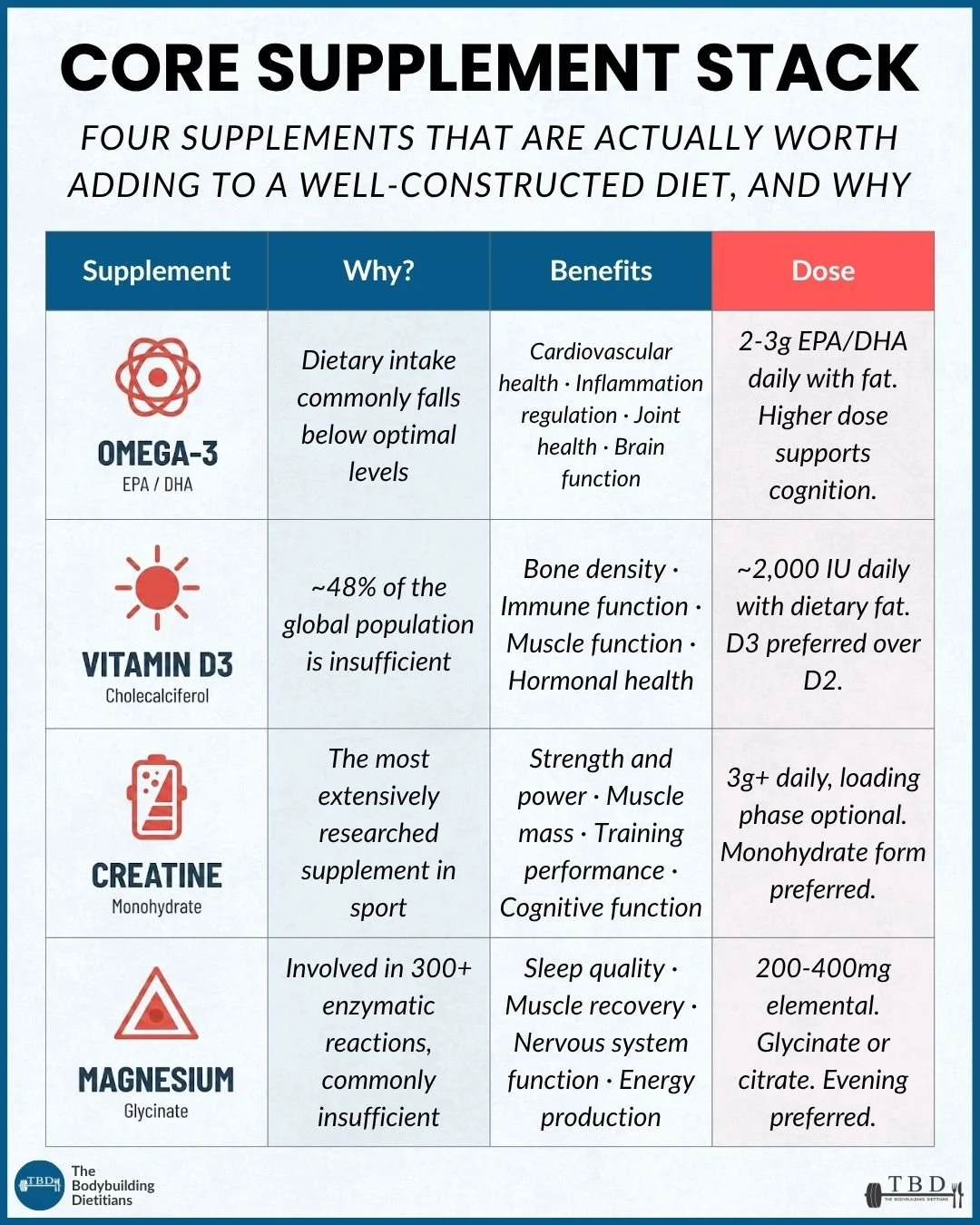
The four supplements with the strongest evidence base for physically active individuals, each addressing a gap that diet alone reliably fails to close.
Most supplements are not worth your money. The supplement industry generates tens of billions of dollars annually by selling products that range from marginally useful to entirely ineffective, often with marketing that dramatically overstates the evidence behind them. For someone trying to make informed decisions about what to spend their money on, the signal-to-noise ratio is genuinely poor.
The four supplements covered in this article make the list because they each meet a specific set of criteria that the vast majority of products on the market do not. Each one addresses a nutrient gap that dietary intake alone reliably fails to close, even in well-constructed diets. Each one has a substantial and consistent body of evidence from randomised controlled trials and meta-analyses supporting its benefits. Each one has a clear, well-established dosing protocol. And each one is relevant to the specific demands of physically active individuals, whether the goal is muscle growth, fat loss, performance, recovery, or long-term health.
This is not a comprehensive list of every supplement that might have some value in specific contexts. There are other products (caffeine, beta-alanine, citrulline, ashwagandha, and others) that have evidence behind them for specific purposes. The four below are the ones that deserve consideration as a baseline stack for most physically active people, because the gap they address is common enough, and the evidence strong enough, that the question is less about whether they are worth taking and more about ensuring the dose, form, and timing are right.
Omega-3 (EPA/DHA): Why It Matters and How to Dose It
Omega-3 fatty acid intake is commonly below optimal levels even among people who eat oily fish regularly, and supplementation with 2 to 3 grams of combined EPA and DHA daily is well supported for cardiovascular health, inflammation regulation, joint health, and brain function.
Omega-3 fatty acids are a family of polyunsaturated fats, the two most physiologically relevant of which are eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). EPA plays a primary role in inflammation regulation and cardiovascular protection, while DHA is a structural component of brain tissue and retinal cells, contributing to cognitive function and neurological health. Both are found predominantly in oily fish (salmon, mackerel, sardines, anchovies) and are poorly converted from the plant-based omega-3, alpha-linolenic acid (ALA), found in flaxseed, chia seeds, and walnuts.
The rationale for supplementation is straightforward. Even among people consuming two or more servings of fatty fish per week, the majority still fall below the omega-3 levels associated with optimal health outcomes. For individuals who eat little or no oily fish, the gap is even larger, and dietary intake alone is very unlikely to meet the levels that the cardiovascular and inflammatory evidence supports.
A meta-analysis of randomised controlled trials examining the effects of omega-3 supplementation on cardiovascular outcomes found that combined EPA and DHA supplementation at doses of 2 to 4 grams per day was associated with significant reductions in cardiovascular events, triglycerides, and inflammatory markers. The benefits were most pronounced at higher doses and in populations with elevated baseline cardiovascular risk or low habitual fish intake.
Source: Hu et al., 2019, Journal of the American Heart Association.
Dosing. The cardiovascular and anti-inflammatory literature supports 2 to 3 grams of combined EPA and DHA daily, taken with a meal containing dietary fat to maximise absorption. For cognitive benefits, emerging research suggests that higher doses (closer to 2 to 3 grams of DHA specifically) may be needed, though the evidence for cognitive outcomes is still developing.
Product selection. When choosing an omega-3 supplement, look for products that specify the EPA and DHA content per serve rather than just total "fish oil," because the total fish oil dose includes fats other than EPA and DHA that do not provide the same benefits. A higher EPA to DHA ratio (approximately 2:1) is generally preferred for anti-inflammatory purposes, as EPA drives the majority of the inflammation-regulatory effects. Triglyceride-form fish oil tends to be better absorbed than ethyl ester form, though both are effective at adequate doses.
For individuals who eat oily fish two to three times per week, a lower supplemental dose (1 to 2 grams of EPA/DHA) may be sufficient to reach optimal levels. For those who eat little or no fish, the full 2 to 3 gram daily dose is more appropriate. In either case, consistency of intake matters more than precision of dosing on any single day.
Vitamin D3 (Cholecalciferol): Why It Matters and How to Dose It
Vitamin D3 is the most prevalent deficiency on this list, with approximately 48% of the global population below the insufficiency threshold. Supplementation at approximately 2,000 IU daily is well supported for bone density, immune function, muscle function, and hormonal health.
Vitamin D functions more like a steroid hormone than a traditional vitamin, influencing the expression of over 1,000 genes after metabolic conversion in the liver and kidneys. Dietary sources (oily fish, eggs, fortified milk) are too limited to reliably maintain optimal levels for most people, particularly during winter months, at higher latitudes, or for individuals with darker skin tones who require more UVB exposure to synthesise vitamin D through the skin.
A meta-analysis of 42 randomised controlled trials found that vitamin D3 supplementation of longer than three years was associated with a statistically significant reduction in all-cause mortality in individuals with baseline levels below 50 nmol/L, and a consistent approximately 15% reduction in cancer mortality. Vitamin D2 supplementation did not replicate these outcomes, supporting the preference for the D3 form.
Source: Zhang et al., 2019, BMJ.
Dosing. A daily dose of approximately 2,000 IU of vitamin D3 is a well-supported starting point for most adults. Individuals with confirmed deficiency (serum 25-hydroxyvitamin D below 50 nmol/L) may benefit from higher initial doses of up to 4,000 IU daily. Baseline blood testing is the most reliable way to determine the appropriate dose and to confirm that supplementation is achieving the target range.
Practical details. Take vitamin D3 with a meal containing dietary fat to maximise absorption. Consider taking it earlier in the day, as emerging evidence suggests evening dosing may interfere with melatonin production and sleep onset. Taking vitamin K2 alongside D3 (particularly at higher doses) helps direct calcium toward bone rather than soft tissue, and many quality products now combine both.
Creatine Monohydrate: Why It Matters and How to Dose It
Creatine is the most extensively researched supplement in sport, with decades of evidence supporting its benefits for strength, power, muscle mass, training performance, and emerging evidence for cognitive function.
Creatine is a naturally occurring compound synthesised from amino acids in the liver, kidneys, and pancreas, and stored primarily in skeletal muscle as phosphocreatine. Phosphocreatine serves as a rapid energy reserve during high-intensity, short-duration efforts (such as heavy resistance training sets) by donating a phosphate group to regenerate ATP, the body's primary energy currency. Supplementation with creatine monohydrate increases intramuscular phosphocreatine stores by approximately 20 to 40%, which extends the capacity for high-intensity work and supports the training quality that drives muscle and strength adaptation over time.
A comprehensive meta-analysis of creatine supplementation and resistance training outcomes confirmed that creatine monohydrate consistently increases lean body mass, strength, and high-intensity exercise performance across a wide range of populations, ages, and training statuses. The effects are dose-dependent and most pronounced when combined with a structured resistance training program.
Source: Forbes et al., 2024, British Journal of Sports Medicine.
The mechanism is worth understanding because it clarifies what creatine does and does not do. Creatine does not build muscle directly. It increases the capacity to perform high-quality training, which is the stimulus that builds muscle. An athlete who supplements creatine but does not train effectively will see no meaningful benefit. An athlete who trains consistently and supplements creatine will be able to sustain higher training quality across sets and sessions, which compounds into greater adaptation over time.
Dosing. 3 to 5 grams of creatine monohydrate daily is sufficient and well established. A loading phase (20 grams per day in divided doses for five to seven days) is sometimes recommended to saturate muscle stores more quickly, but it is optional. Daily dosing at 3 to 5 grams will achieve the same saturation within approximately three to four weeks without the gastrointestinal discomfort that loading can sometimes produce.
Form selection. Creatine monohydrate is the preferred form. It is the most extensively researched, the most cost-effective, and consistently performs as well as or better than more expensive alternatives (creatine HCL, buffered creatine, creatine ethyl ester). There is no evidence supporting the superiority of any alternative form over monohydrate for strength, performance, or body composition outcomes.
Cognitive benefits. There is emerging evidence that creatine supplementation may support cognitive function, particularly under conditions of sleep deprivation, mental fatigue, or high cognitive demand. The doses studied for cognitive outcomes tend to be higher than those used for performance (closer to 10 grams per day in some studies), and more research is needed before specific dosing recommendations for cognitive benefits can be made with confidence. For now, 10 grams per day is a reasonable exploratory dose for those interested in the cognitive applications, while 3 to 5 grams remains the well-established dose for performance.
Timing. Creatine does not need to be timed around training. Daily intake at any consistent time is sufficient, because the benefit comes from maintaining saturated intramuscular stores over time rather than from acute effects of a single dose. Taking it with a meal may improve absorption marginally, but the effect of timing on outcomes is negligible.
Common concerns. Creatine does not cause kidney damage in healthy individuals, does not cause hair loss (the single study that suggested a link to DHT has not been replicated), and does not cause dehydration. It does cause a modest increase in body weight (typically 1 to 2 kilograms) due to increased intracellular water retention in muscle, which is a normal and expected effect that reflects increased muscle hydration rather than fat or subcutaneous water gain.
Magnesium (Glycinate): Why It Matters and How to Dose It
Magnesium is involved in over 300 enzymatic reactions in the body and is commonly insufficient in people with high training loads, making it one of the most practically relevant supplements for active individuals, particularly for its effects on sleep quality, recovery, and nervous system function.
Magnesium is the fourth most abundant mineral in the body and a cofactor for enzymes involved in energy production (ATP synthesis), protein synthesis, muscle and nerve function, blood glucose regulation, and bone metabolism. For physically active individuals, magnesium is relevant through two primary pathways: its role in muscle contraction and recovery, and its influence on sleep quality through interaction with the parasympathetic nervous system and GABA receptors.
The rationale for supplementation is that dietary magnesium intake is commonly below recommended levels, even in well-structured diets. The richest food sources (pumpkin seeds, almonds, dark chocolate, spinach, black beans) are not always well-represented in physique-focused nutrition plans, and exercise increases magnesium requirements by 10 to 20% through increased urinary and sweat losses. The combination of higher demand and potentially insufficient intake creates a common gap that supplementation can reliably address.
A systematic review of magnesium supplementation and sleep quality found that magnesium supplementation was associated with improvements in subjective sleep quality, sleep onset latency, and sleep duration, particularly in individuals with low baseline magnesium status. The effect was most consistently observed with supplementation doses of 200 mg or more of elemental magnesium, taken in the evening.
Source: Arab et al., 2023, BMC Complementary Medicine and Therapies.
Dosing. 200 to 400 mg of elemental magnesium daily is the well-supported range. "Elemental" magnesium refers to the actual magnesium content of the supplement, as opposed to the total weight of the compound (for example, a 2,000 mg magnesium glycinate capsule may contain only 200 mg of elemental magnesium, with the remainder being the glycine molecule it is bound to). Checking the elemental magnesium content on the label is important for ensuring the dose is appropriate.
Form selection. The form of magnesium matters significantly for both absorption and tolerability. Magnesium glycinate (also labelled as bisglycinate) is the preferred form for most people because it is well-absorbed, gentle on the gastrointestinal system, and the glycine component has calming properties that complement the sleep-supporting effects of magnesium. Magnesium citrate is also well-absorbed and can have a mild laxative effect, which may be an additional benefit for individuals who experience constipation. Magnesium oxide, the cheapest and most widely available form, has significantly lower bioavailability and is more likely to cause gastrointestinal discomfort, making it a less effective choice despite its lower cost.
Timing. Evening dosing is preferred, supported by the sleep quality literature and consistent with the calming effects of both magnesium and glycine on the nervous system. Taking magnesium glycinate 30 to 60 minutes before bed is a practical routine that aligns with both the evidence and sleep hygiene strategies.
How Does This Stack Fit Within a Broader Nutrition Plan?
These four supplements are designed to complement a well-constructed diet, not to replace one. They address specific gaps that dietary intake alone commonly fails to close, but they do not compensate for a poor overall dietary pattern.
The hierarchy of importance for body composition and health outcomes remains: total calorie intake, macronutrient distribution, food quality and diversity, micronutrient adequacy from whole foods, meal timing and distribution, and then supplementation. Supplements occupy the final layer of that hierarchy, which means their incremental benefit is meaningful only when the layers beneath them are already well-managed.
For someone whose diet is poorly constructed (insufficient protein, inadequate fibre, narrow food diversity, chronic energy imbalance), the return on investment from supplementation will be marginal regardless of how well the stack is designed. For someone whose diet is well-constructed and who is training consistently, these four supplements close the most common remaining gaps and provide a meaningful return for a relatively modest cost.
This is the approach that our coaching takes to supplementation: recommending products strategically based on individual diet, blood work, and context rather than applying a blanket protocol. For some clients, all four supplements are appropriate. For others, one or two may be sufficient, and the money saved on unnecessary products is better spent on food quality. The right stack depends on the individual.
What About Other Supplements?
The supplement industry offers hundreds of products marketed to active individuals, and many of them have some evidence behind them for specific purposes. A few worth acknowledging briefly:
Caffeine is one of the most well-evidenced performance-enhancing supplements available, with consistent benefits for strength, endurance, and cognitive performance at doses of 3 to 6 mg per kilogram of bodyweight. It is not included in this core stack because most people already consume caffeine through coffee, tea, or pre-workout supplements, and the question of whether to supplement it is typically about timing and dose management rather than whether to take it at all.
Protein powder (whey, casein, or plant-based isolates) is a practical tool for meeting protein targets, but it is a food product rather than a supplement in the traditional sense. Its value lies in convenience rather than in any unique physiological effect that whole food protein sources cannot provide.
Beta-alanine has evidence for improving performance in sustained high-intensity efforts (60 to 240 seconds), but its benefit is specific to certain training contexts and may not be relevant for everyone.
Ashwagandha has emerging evidence for stress modulation, sleep quality, and potentially testosterone in specific populations, but the evidence base is less robust and less consistent than the four supplements covered above.
None of these are categorically bad choices, but none meet the same threshold of universally relevant, evidence-strong, common-gap-addressing supplementation that omega-3, vitamin D3, creatine, and magnesium do. The four covered in this article form a practical baseline; additional products can be layered on top based on individual needs, goals, and the guidance of a qualified professional.
If you would like personalised guidance on which supplements are appropriate for your situation, based on your current diet, training, blood work, and goals, a consultation with one of our dietitians can help you build a targeted, cost-effective protocol.
Practical Takeaways
Most supplements are not worth your money. Omega-3, vitamin D3, creatine monohydrate, and magnesium glycinate are the four with the strongest evidence base for physically active individuals, each addressing a gap that diet alone commonly fails to close.
Omega-3: take 2 to 3 grams of combined EPA and DHA daily with a fat-containing meal. Choose products that specify EPA and DHA content per serve, and favour a higher EPA to DHA ratio (approximately 2:1) for anti-inflammatory benefits.
Vitamin D3: take approximately 2,000 IU daily with dietary fat, earlier in the day. D3 is preferred over D2. Baseline blood testing guides the appropriate dose and confirms whether supplementation is achieving the target range.
Creatine monohydrate: take 3 to 5 grams daily at any consistent time. No loading phase is required, monohydrate is the preferred and most cost-effective form, and timing relative to training does not meaningfully affect outcomes.
Magnesium glycinate: take 200 to 400 mg of elemental magnesium in the evening, 30 to 60 minutes before bed. Glycinate is preferred over oxide for absorption and tolerability, and evening dosing aligns with the sleep quality evidence.
Supplements complement a well-constructed diet but do not replace one. Their benefit is meaningful only when overall calorie intake, macronutrient distribution, food quality, and micronutrient adequacy from whole foods are already well-managed.
Frequently Asked Questions
What are the best supplements for building muscle?
Creatine monohydrate is the supplement with the strongest evidence for supporting muscle growth, primarily through its effect on training quality rather than a direct muscle-building mechanism. Beyond creatine, ensuring adequate vitamin D status (which supports muscle protein synthesis and hormonal function) and sufficient omega-3 intake (which supports recovery and inflammation regulation) contribute to the physiological environment in which muscle growth occurs. Protein powder is also useful as a practical tool for meeting protein targets.
Is creatine safe to take every day?
Creatine monohydrate is one of the most extensively studied supplements in sport and has been consistently demonstrated to be safe for daily long-term use in healthy individuals. It does not cause kidney damage, dehydration, or hair loss in populations without pre-existing conditions. The modest weight gain (1 to 2 kilograms) associated with creatine use reflects increased intracellular water in muscle tissue, not fat gain.
Should you take omega-3 if you eat fish?
Even among people who eat two or more servings of oily fish per week, the majority still fall below the omega-3 levels associated with optimal cardiovascular and inflammatory outcomes. If you eat oily fish regularly, a lower supplemental dose (1 to 2 grams of EPA/DHA) may be sufficient. If your fish intake is infrequent or absent, the full 2 to 3 gram daily dose is more appropriate.
What form of magnesium is best?
Magnesium glycinate (bisglycinate) is the preferred form for most people because of its superior absorption, gastrointestinal tolerability, and the calming properties of the glycine component. Magnesium citrate is a well-tolerated alternative with a mild laxative effect. Magnesium oxide, while the cheapest and most widely available, has significantly lower bioavailability and is more likely to cause gastrointestinal discomfort, making it less effective despite its lower cost.
Do you need a loading phase for creatine?
A loading phase (20 grams per day in divided doses for five to seven days) can saturate muscle creatine stores more quickly, but it is not necessary. Daily dosing at 3 to 5 grams will achieve the same saturation level within approximately three to four weeks. Many people prefer to skip the loading phase to avoid the gastrointestinal discomfort that higher doses can sometimes produce.
When should you take vitamin D?
Vitamin D3 should be taken with a meal containing dietary fat to maximise absorption, as it is a fat-soluble nutrient. Taking it earlier in the day (with breakfast or lunch) is recommended because emerging evidence suggests that evening dosing may interfere with melatonin production and sleep onset. Blood testing for serum 25-hydroxyvitamin D is the most reliable way to determine whether the current dose is achieving adequate levels.
If you would like personalised supplement recommendations based on your current diet, training, blood work, and goals, our team of dietitians can help you build a targeted, evidence-based protocol.